Okay. In the last post I mentioned that I get annoyed when concerns about opioids being diverted pop up in discussions about when opioids are indicated treatments. It's not that I don't think diversion is an important concern in drug policy. It's just that I feel like it shouldn't be part of discussions of when opioids are good treatments.
Anyway, I was annoyed by not knowing I feel this way.* So, the following is some off-the-cuff noodling about when concerns are relevant in decisions about the use of opioid drugs. I'm not at all sure about how much of it I want to stand behind. But hopefully it might be useful for sparking some discussion.
*I remember someone once telling me that philosophy starts with a sense of wonder. I have since found that, for me, it usually starts with annoyance; it ends in wonder.
-------------
In general, I tend to think that the dangers of opioid diversion --opioids ending up outside of the patient's hands-- get too much weight in discussions of drug policy (although some recent statistics on overdose and death rates involving opioids are giving me some pause in my beliefs about the severity of diversion's harms).
But in addition to questions about how severe the consequences of diversion are, we also need to know whose problem it is. A comprehensive drug policy spans many different areas including, inter alia, the law in its criminal, civil, and regulatory forms; professional determinations of best clinical practices; and individual clinicians' decisions about how to treat individual patients. Thus we need to know whether preventing diversion should have the same importance for everyone involved in the prescription drug arena.
I'm going to suggest that preventing diversion can be a legitimate concern at the more general levels. And they may inform doctors practices in a general way. But, I suspect, the potential harms resulting from diversion should not factor into a doctor's decisions about what medications to prescribe a patient.
My claims here will rest on the supposition that a clinician's ethical responsibilities arise from her patient's individual welfare. Her professional obligation is not the promotion of the general welfare via her interactions with a certain individual. The clinician's responsibility is to alleviate her patient's suffering in the safest and most effective way available.
A rough analogy may help bring out this distinction between duties based in the promotion of the general welfare and duties based in the promotion of an individual's welfare. In an adversarial system of criminal justice like we have in the United States, the role of a defense attorney is to advocate for her clients interests as best she can. Even if she recognized that her client's conviction may benefit the public at large, she is obligated to ignore that fact in doing her job. This doesn't mean that the job of defense attorney is entirely removed from the enterprise of promoting the public good. It's that a system in which a party is assigned to look out only for the interests of the defendant is more likely to be better overall. (One major disanalogy here is that my supposition about the source of the doctor's duties need not appeal to claims about what would best promote the general welfare.)
If we a clinician's duties as tied her patient's welfare in this way, concerns about the welfare of others are thus (nearly always) irrelevant to decisions about what substances to prescribe her patient. This suggests that even though the clinician may foresee that others may be harmed through diversion if she prescribes an opioid to a patient, this possibility should have no weight in her decision about what to prescribe. Her duty arises from and is directed at the health of her patients, not the health of people in general.
Obviously, this has its limits. Massive harms to others may trump this obligation. And it may be that if two treatments were exactly equal in their efficacy and safety, then considerations of the general good or other effects on others may break the tie.
Nor does this mean that the doctor must completely ignore the possibility that the drug will be diverted. Other public entities' interests in preventing diversion are based in their obligation to protect public health overall. But given the source of her professional obligations, the clinician's concerns about diversion should be limited to its effects on her patient's health.
Clearly, a responsible clinician must be attuned to the possibility that the patient herself will divert the drug. But her vigilance is not demanded by the need to prevent harms to the recipients of the diversion. It comes from her responsibilities to the patient. The clinician's treatment decisions must be based on the supposition that the patient will comply with the prescribed regime. She cannot aim to promote an individual's welfare by prescribing her a substance that she believes that the patient will not take. Therefore, the belief that the patient will take the drug as prescribed is a necessary condition of justifiably prescribing an opioid.
Suppose that a patient is accompanied by a stoned adolescent whose T-shirt reads "I love drugs!" Does this necessary condition imply that she ought to take into consideration the likelihood that the son will divert the drugs?
The answer seems to be yes. She cannot prescribe a medication to benefit her patient if she believes that the patient won't take the drug because someone else will steal it. Of course, it's unlikely that the suspicion in this case would justify her refusing to prescribe an otherwise indicated opioid Much will hang on the strength of her conviction that the drug will be diverted. In the drug diverting adolescent case, the clinician may be required to put special emphasis on the need to keep control of the medication in counseling the patient. But as long as she can be satisfied that the patient will be reasonably vigilant, she will be justified in writing the prescription. Her uncertainty about the likelihood of diversion combined with the need to respect the patient's autonomy will set the bar for reasonable vigilance pretty low.
Cases in which she should altogether refuse to prescribe on these grounds will likely be rare. But they are easy to imagine. Suppose that a disabled patient is completely dependent on her caretaker for all of her medications. If the clinician was convinced that the caretaker would divert a significant portion of the prescribed opioid, then she should not write the prescription. Indeed, doing so would be tantamount to writing the prescription for the caretaker. Though, she may have some obligation to seek other ways of getting the indicated treatment to the patient (e.g., recommending at home nursing visits, and patient treatment).
What's important is the way concerns about diversion are figuring in here. A clinician should be cautious of diversion insofar as it would interfere with her patient's treatment. Her responsibilities do not depend on how the recipients of the diverted substance may be affected. Those dangers of diversion give her reason to, for example, keep her cabinets locked. But they should be irrelevant to her decisions about patients' treatments.
This is not to say that a comprehensive drug policy should not be concerned about the harms to non-patients who gain access to opioids through diversion. It is a fact that the availability of opioids in legitimate channels will involve some diversion and some non- patients will be harmed. While the clinician's responsibility is based in her individual patient's welfare, government policies are properly attuned to protecting welfare across the board. Thus entities (in the US) like the FDA, the Department of Justice and the DEA are justified in creating policies and enforcement practices which will minimize the amount of diversion.
But this picture of the clinician's obligations does create tension between the government's proper aims creating drug policy and the duties of clinicians. We should thus want a principled way of resolving these kinds of inevitable conflict. One possibility is that one set of considerations will always trump the other (that is, the first set is lexically prior to the other).
To see the implications of a lexical ordering of these considerations suppose that the paramount consideration in shaping drug policy was ensuring clinicians' abilities to carry out their duties to their patients. This would have implications for how we decide conflicts. Such a partial lexical ordering would entail that the protection of access to safe and effective drugs cannot be trumped by considerations about diversion. More generally, this might mean that any proposed policy that would promote the general good could be vetoed if it unreasonably affected the ability of clinicians to treat their patients.
This ordering of concerns would be unlikely to undermine reasonable restrictions on the use and prescription of opioids. For example, this is compatible with a well regulated and organized system for inventory control in the manufacturing, shipping, and distribution of opioids. The same is true for methods of verifying the legitimacy of prescriptions and the identity of patients. But some apparently relatively mild restrictions on prescribing ability may not be compatible with this set of drug policy priorities.
For example, the FDA is presently considering requiring all clinicians who prescribe powerful long-acting opioids to have a special certification. Many general practice clinicians who currently prescribe such medications may be unwilling to go through the hassle of obtaining and maintaining the certification. If the certification process was unduly difficult, many clinicians would be unable to prescribe the medications that they thought were best indicated for their patients conditions. Such a regulation would likely decrease the number of deaths from diversion. But no matter how many diversion related deaths would be prevented, it should be rejected if we believe that the clinician's abilities to treat their patients should always trump any other consideration.
So, in sum, here's what I've suggested: If we think about the source and nature of clinicians' professional obligations in a particular way, then concerns about diversion should not play a role in determining whether to prescribe an opioid (outside of diversion undermining the treatment regime). Direct focus on preventing diversion is instead the job of regulatory agencies whose mission is the common public good.
I haven't given any argument in favor of the further idea that concerns about diversion should always be subordinated to clinicians ability to prescribe opioids as they see fit. Though I am definitely attracted to this view. We can leave that a subject for another post.
25 June 2009
Opioids often preferable to NSAID's in the elderly
This is important.
The NYT reports that in light of findings that
The American Geriatrics Society
Editorial comment: I'm unhappy that the reporter chose to use this quote in emphasizing that opioids have their own dangers:
Diversion of opioids is a real problem. But it really annoys me to see it used as a counterpoint in discussions of their clinical usefulness.
I almost feel like these claims are saying something like: Advil might kill Grandma, but we might not want to give her a safer treatment because her grandson might steal it and kill himself.' (I don't think the reporter or Dr. Chou intended it this way --that's just how I take it)
Update: I was bothered by not knowing why the stuff about diversion annoys me so much. So I've posted some very rough thoughts here.
The NYT reports that in light of findings that
[in elderly patients] The risks of Nsaids include ulcers and gastrointestinal bleeding and, with some drugs, an increased risk of heart attacks or strokes. The drugs do not interact well with medicines for heart failure and other conditions, and may increase high blood pressure and affect kidney function, experts said.
The American Geriatrics Society
removed those everyday medicines, called Nsaids, for nonsteroidal anti-inflammatory drugs, from the list of drugs recommended for frail elderly adults with persistent pain. The panel said the painkillers should be used “rarely” in that population, “with extreme caution” and only in “highly selected individuals.”
[....]
“We’ve come out a little strong at this point in time about the risks of Nsaids in older people,” said Dr. Bruce Ferrell, a professor of geriatrics at U.C.L.A. who is chairman of the panel. “We hate to throw the baby out with the bathwater — they do work for some people — but it is fairly high risk when these drugs are given in moderate to high doses, especially when given over time.
“It looks like patients would be safer on opioids than on high doses of Nsaids for long periods of time,” he continued
Link (My italics; I've interpolated the order of the paragraphs)
Editorial comment: I'm unhappy that the reporter chose to use this quote in emphasizing that opioids have their own dangers:
“We’re seeing huge increases nationwide of reports about the misuse and diversion of prescription drugs and related deaths,” said Dr. Roger Chou, a pain expert who was not involved in writing the guidelines for the elderly but directed the clinical guidelines program for the American Pain Society. “The concerns about opioids are very real.”
Diversion of opioids is a real problem. But it really annoys me to see it used as a counterpoint in discussions of their clinical usefulness.
I almost feel like these claims are saying something like: Advil might kill Grandma, but we might not want to give her a safer treatment because her grandson might steal it and kill himself.' (I don't think the reporter or Dr. Chou intended it this way --that's just how I take it)
Update: I was bothered by not knowing why the stuff about diversion annoys me so much. So I've posted some very rough thoughts here.
16 June 2009
Resources for Causalgia (CRPS/RSD)
Here's a helpful guide to resources on Complex Regional Pain Syndrome/Reflex Sympathetic Dystrophy (CRPS/RSD/Causalgia)
For those of you who don't know, Causalgia (CRPS/RSD) should rank high on the list of 'Things-You-Don't-Want'.
On the IASP definition:
Or as it was first described by Silas Weir Mitchell in 1872 after the Civil War
In other words, in causalgia part of your body feels like it's constantly on fire.
Resources and Relief for Reflex Sympathetic Dystrophy
For those of you who don't know, Causalgia (CRPS/RSD) should rank high on the list of 'Things-You-Don't-Want'.
On the IASP definition:
Causalgia
A syndrome of sustained burning pain, allodynia, and hyperpathia after a traumatic nerve lesion, often combined with vasomotor and sudomotor dysfunction and later trophic changes.
Or as it was first described by Silas Weir Mitchell in 1872 after the Civil War
"We have some doubt as to whether this form of pain ever originates at the moment of the wounding. . . Of the special cause which provokes it, we know nothing, except that it has sometimes followed the transfer of pathological changes from a wounded nerve to unwounded nerves, and has then been felt in their distribution, so that we do not need a direct wound to bring it about. The seat of the burning pain is very various; but it never attacks the trunk, rarely the arm or thigh, and not often the forearm or leg. Its favorite site is the foot or hand. . . Its intensity varies from the most trivial burning to a state of torture, which can hardly be credited, but reacts on the whole economy, until the general health is seriously affected....The part itself is not alone subject to an intense burning sensation, but becomes exquisitely hyperanesthetic, so that a touch or tap of the finger increases the pain." quoted in UCLA pain exhibit
In other words, in causalgia part of your body feels like it's constantly on fire.
Online introduction to pain processes
The-New-Science-of-Pain-Relief has a nice introductory walkthrough of the basic neurology of pain here.
Philosophers will, of course, carefully take note the role of C nociceptive afferents.
Philosophers will, of course, carefully take note the role of C nociceptive afferents.
11 June 2009
ABC story on FDA Acetaminophen overdose report
With every changing of the seasons comes a new set of cautions about acetaminophen use.
Like the changing of the leaves, experts call for better public education and packaging practices.
And, like the migration of the butterflies^, the pharmaceutical industry tells them to go f*** themselves:
See this show again in a few months and a couple thousand more deaths.
^Sorry for the bad simile
Like the changing of the leaves, experts call for better public education and packaging practices.
And, like the migration of the butterflies^, the pharmaceutical industry tells them to go f*** themselves:
McNeil Consumer Healthcare, a Johnson & Johnson subsidiary and the manufacturer of Tylenol, said in a statement Thursday that they fear the [FDA report's] recommendations could have the effect of steering consumers away from an appropriate and safe drug.
"While we share the FDA's mutual goal of preventing and decreasing the misuse and overdose of acetaminophen, we have concerns that some of the FDA recommendations could discourage appropriate use and are not necessary to addressing the root causes of acetaminophen overdose," the statement reads. Link
See this show again in a few months and a couple thousand more deaths.
^Sorry for the bad simile
Pain in animal slaughter
Newsflash!
Cutting calves throats hurts, study says...
Cutting calves throats hurts, study says...
N Z Vet J. 2009 Apr; 57(2): 74-6
Mellor DJ, Gibson TJ, Johnson CBCommercial slaughter of farm livestock usually employs an extensive incision that severs the soft tissues of the neck including the major blood vessels supplying and draining the brain. It is intended to cause a catastrophic decrease in cerebral blood flow with rapid onset of unconsciousness or insensibility. The tissues of the neck are innervated with nociceptive nerve fibres and their transection will cause a barrage of sensory impulses. Consciousness, and therefore the ability of the animal to feel pain and experience distress after the incision, may persist for 60 seconds or longer in cattle. These observations suggest that livestock may experience pain and distress during the period before they become unconscious (insensible). Psychological shock and fear may also be associated with the extensive tissue damage and blood loss. Pre-incision stunning has been adopted as a precautionary measure to prevent suffering. However, the question remains: How intense and noxious are these experiences? Recent methodological developments related to quantitative analysis of the electroencephalogram (EEG) allow the experience of pain to be assessed more directly than has hitherto been possible. This methodology has now been applied to the question of the slaughter of calves by ventral-neck incision. The new information demonstrates clearly for the first time that the act of slaughter by ventral-neck incision is associated with noxious stimulation that would be expected to be perceived as painful in the period between the incision and loss of consciousness. These data provide further support for the value of stunning in preventing pain and distress in animals subjected to this procedure."
(Via HubMed - pain.)
Obstetric anesthesia: Past present and future.
And yet another addition to my never ending reading list.
Obstetric anesthesia: Past present and future.: "
J Matern Fetal Neonatal Med. 2009 Jun 1; 1-4
Kuczkowski KMObstetric anesthesia is science and art combined, and obstetric anesthesiologists must be concerned simultaneously with the lives of (at least two) intricately interwoven patients - the mother and her baby (ies). Obstetric anesthesia, by definition, is a subspecialty of anesthesia devoted to peripartum, perioperatvie, pain and anesthetic management of women during pregnancy and the puerperium. Perhaps no other subspecialty of anesthesiology provides more personal gratification than the practice of obstetric anesthesia. An obstetric anesthesiologist has become an essential member of the peripartum care team, who closely works with the obstetrician, perinatologist, midwife, neonatologist and labor and delivery nurse to ensure the highest quality care for the pregnant woman and her baby. Exchange on information and communication skills in ever changing environment of labor and delivery is essential for perfect outcome, which is always expected when providing safe passage for both the mother and her fetus from antepartum to postpartum period. Changes in maternal-fetal and neonatal medicine and obstetric anesthesia have continued to develop rapidly during the recent years. The purpose of this article is to explore a number of important issues in modern practice of obstetric anesthesia."
(Via HubMed - pain.)
Effect of mental stress on cold pain in chronic tension-type headache sufferers.
Here's a little bit about headache and stress.
Effect of mental stress on cold pain in chronic tension-type headache sufferers.: "
J Headache Pain. 2009 Jun 5;
Cathcart S, Winefield AH, Lushington K, Rolan PMental stress is a noted contributing factor in chronic tension-type headache (CTH), however the mechanisms underlying this are not clearly understood. One proposition is that stress aggravates already increased pain sensitivity in CTH sufferers. This hypothesis could be partially tested by examining effects of mental stress on threshold and supra-threshold experimental pain processing in CTH sufferers. Such studies have not been reported to date. The present study measured pain detection and tolerance thresholds and ratings of supra-threshold pain stimulation from cold pressor test in CTH sufferers (CTH-S) and healthy Control (CNT) subjects exposed to a 60-min stressful mental task, and in CTH sufferers exposed to a 60-min neutral condition (CTH-N). Headache sufferers had lower pain tolerance thresholds and increased pain intensity ratings compared to controls. Pain detection and tolerance thresholds decreased and pain intensity ratings increased during the stress task, with a greater reduction in pain detection threshold and increase in pain intensity ratings in the CTH-S compared to CNT group. The results support the hypothesis that mental stress contributes to CTH through aggravating already increased pain sensitivity in CTH sufferers."
(Via HubMed - pain.)
Acupuncture And Pain
In answer to a reader's question, How To Cope With Pain digs up some conclusions about the efficacy of acupuncture.
Acupuncture And Pain: "An excellent review article by Edzard Ernst, M.D., reports that the conditions that are most solidly backed up by evidence showing acupuncture helps are:
- chemotherapy-induced nausea/vomiting
- postoperative nausea/vomiting
- idiopathic headache (headache of unknown cause)
Many other diseases, both pain-related and not, were not helped by acupuncture. Ernst concludes that studies ‘do not suggest that this treatment is effective for a wide range of conditions.’"
[Read the rest for some limitations in the current literature]
The original article is Acupuncture: What does the most reliable evidence tell us?, in the Journal of Pain and Symptom Management 2009, Vol 37, pages 709-714.
(Via How To Cope With Pain Blog.)
Palliative care for a patient with anorexia nervosa
Pallimed brings up a very hard case. I'm honestly not sure what I think about much of this:
Palliative care & eating disorders: "The International Journal of Eating Disorders has a case report and discussion of a patient with refractory anorexia nervosa who died receiving hospice care. This is one fascinating case report. The case, to summarize briefly, involved a young woman with a long history of anorexia nervosa, refractory to all attempts at treatment (including involuntary/forced treatment) who apparently also was not deemed a candidate for forced guardianship (the hospital's legal counsel advised she would not meet requirements to be declared incompetent).
This is how they describe the ethics committee's response to the case:The committee’s members struggled to understand how one could die from a psychiatric illness (other than by suicide or unintentional overdose) and were not sure how to proceed. Although they could delineate the differences between acute mental health risks such as suicide, drug overdoses, psychosis or self-neglect, they had no points of reference regarding how to manage a patient who was chronically a danger to herself, unwilling to engage in further treatments, and unresponsive to all prior attempts to treat her involuntarily. The only examples the committee raised for comparison concerned drug users who received heart valve replacements, yet continued to use, knowing that such ongoing use would kill them. In such cases, if a high risk of ongoing subsequent IV drug use was suspected ahead of time, the decision was often made not to provide valve replacements, but there was no forced treatment.This is how they presented what palliative care for anorexia nervosa would look like to the patient (italics mine):If she chose to pursue treatment she would be assisted, but the staff would not force her into any involuntary placements or impose any treatment she did not want. There would be no weigh-ins, no calorie or exercise monitoring, no IM medications and no required therapy sessions. She would be offered outpatient therapy only as she felt desirable and necessary. Psychiatric medications would be prescribed as the patient deemed necessary to help manage depression, anxiety and insomnia. The patient would receive weekly visits from a palliative care nurse, who would work with her to manage her symptoms and keep her comfortable. The patient agreed to no further hospitalizations, but did not fully agree with the plan for ‘‘palliative care’’ since she did not believe she was going to die.The patient basically continued her illness behaviors, got weaker/sicker, and was eventually enrolled in an inpatient hospice where she died.
Some observations.
- AN is clearly at times a terminal illness, refractory to all attempts to reverse it.
- In this case it was clear that the patient's life could have been prolonged although only with forced treatment. It was the opinion of her physicians that such forced treatment, while life-prolonging, would not 'cure' her AN (for some patients a trial, or many trials, of forced nutritional treatment along with psychiatric care gets them to the point at which they are willing to continue with voluntary treatment and can have a durable response; it was felt this would never happen with this patient). Thus the decision came down to trying to force further involuntary treatment vs. letting the disease run its natural course with her inevitably dying.
- I found it interesting that they did not feel there was enough of a chance she'd be considered incompetent that they didn't even put her through the court process. Her statement that she did not think she would die (and it seems she continued that belief until the end, and persisted at least until she was enrolled in hospice in saying that she in fact wanted to live) seems to me to indicate such a fundamental lack of insight into her condition that I'm not sure I believe that. Granted, I'm not too familiar with criteria for declaring someone incompetent on psychiatric grounds, but I assume it has something to do with one's mental illness being such that one cannot even take in basic medical information.
- That said, and even if she was legally stripped of her decision-making rights, for situations in which even involuntary treatment would not work long-term, is it right to force patients to do that? In this situation they concluded No, and made plans accordingly, which seemed to work as well as could be expected under the circumstances.
[A very interesting discussion follows in the rest. Definitely give it a read]
Treating Psychiatric Symptoms
From the How To Cope With Pain Blog, here's a bit about the role of a psychiatrist in comprehensive pain management:
Treating Psychiatric Symptoms: "
Welcome to the continuing series Why You Should See a Pain Management Psychiatrist. Last week we learned that psychiatric symptoms - such as depression, anxiety, etc. - often accompany chronic pain. This week we’ll look at how to treat psychiatric diseases.
As we saw, depression (8-50% of patients with pain), anxiety (19-50%), PTSD (10%), sleep disturbance (50% or more), drug and alcohol problems (3-19%) are common in patients with pain. Let’s look at some important issues related to treating these problems.
1. Identifying symptoms
To be able to treat psychiatric symptoms, they first have to be identified. Your doctor should be asking about these common symptoms and referring you if appropriate. You should also report if you’re having such symptoms. Don’t be embarrassed or feel like you’re complaining. Getting help is important!
2. Taking symptoms seriously
If you’re having significant depression, anxiety or other symptoms, it’s important to report these to start to get treatment for them. These symptoms should not be dismissed as, ‘of course you have depression - it’s because of your pain.’ Chronic pain does not automatically mean depression, anxiety and disturbed sleep. There’s treatment for these symptoms.! And they should be treated!
3. Treat all the disorders that are present.
We know that if psychiatric problems are present along with pain, it’s crucial to treat both. Treating just 1 doesn’t make the other go away. For example, if someone has depression and pain, treating just pain doesn’t necessarily mean the depression will go away. And sometimes neither gets better unless you treat both.
4. Treatment
There are both therapies and medications to treat nearly all psychiatric diseases. Medication should be used only along with therapy. I strongly recommend trying therapy first, before medication, to see if just therapy alone can work. There are times, when psychiatric symptoms are severe, that both will be started at once, but that’s less common. Most people with pain disorders are already on several medications and sometimes already tolerating side effects, so trying non-medication treatment first makes sense.
Other articles in the series:
"
- Why comprehensive treatment works better
- Benefits of a psychiatric evaluation
- Treatment of psychiatric symptoms
- Using psychiatric medications for pain
- Learning psychological skills
- Making positive behavioral changes
- Making positive psychological changes
- Benefits of supportive therapy
- Benefits of a pain support group
- New brain-based treatments
(Via How To Cope With Pain Blog.)
Refusal to torture in Milgram experiments
Oh well. From Brain Blogger, a new experiment which deflates some of the hope for humanity I had held out in the face of the Milgram experiments on torture and obedience to authority:
Though I think Dr. Surve is reaching quite a bit in concluding that
The first sentence gets some support from the experiment. I don't see why the second would.
Not that that's much consolation.
For the first time in over 30 years, a scientist named Dr. Jerry Burger managed to obtain approval for a study partially reproducing the Milgram experiment, and in 2009 he published his findings in the journal American Psychologist....Dr. Burger also had some subjects witness a planted tester who refused to administer the test. He hypothesized that seeing a prior refusal might embolden test subjects to also refuse. Nevertheless, Dr. Burger’s results were comparable to Dr. Milgram’s results, and having a witnessed refusal did not significantly change [the willingness of subjects to continue increasing the voltage of the shocks].
References
Burger, J. (2009). Replicating Milgram: Would people still obey today? American Psychologist, 64 (1), 1-11 DOI: 10.1037/a0010932
Though I think Dr. Surve is reaching quite a bit in concluding that
Whatever moral compass human beings claim to possess, this research suggests that when presented with a perceived authority figure, the majority will override that compass in favor of obedience. The only possible conclusion, then, is that most human beings are in fact hard-wired to torture.
The first sentence gets some support from the experiment. I don't see why the second would.
Not that that's much consolation.
Sphenopalatine ganglioneuralgia (aka Brain Freeze)
Brain Blogger has a primer here.
It's based on this article:
Kaczorowski, M. (2002). Ice cream evoked headaches (ICE-H) study: randomised trial of accelerated versus cautious ice cream eating regimen. BMJ, 325(7378), 1445-1446. DOI: 10.1136/bmj.325.7378.1445
Sigh. I must be in the wrong field. Not much ice cream related research in philosophy.
It's based on this article:
Kaczorowski, M. (2002). Ice cream evoked headaches (ICE-H) study: randomised trial of accelerated versus cautious ice cream eating regimen. BMJ, 325(7378), 1445-1446. DOI: 10.1136/bmj.325.7378.1445
Sigh. I must be in the wrong field. Not much ice cream related research in philosophy.
Migraines
From Brain Blogger Dr. Shaheen Lakhan's interview with headache expert Dr. Roger K Cady, a bit about the current understanding of what migraines are:
Read the whole thing here
Shaheen Lakhan: To start off, what sets a migraine apart from a tension-type headache?
Roger Cody: ...tension headache is a headache without the presence of other symptoms. The headache is generally mild to moderate in intensity, more likely to be on both sides of the head and with a steady and pressure quality to the pain. It is not associated with nausea or sensitivity to light or sound.
Migraine is the most common headache causing people to seek medical attention. Migraine is always more than just a headache. The headache can be on one or both sides of the head and more likely to have a throbbing quality or to be made worse by daily activity or things like bending over. Associated with the headache are symptoms like nausea and sensitivity to light, sound, and other sensory stimuli.
[....]
In people with migraine, many experts suggest that migraine and tension headaches exist on the same spectrum and arise out of the same pathophysiological process (big and little migraines).
SL: I recall the vascular theory of migraine from decades past which held that migraine symptoms were a function of ischemia and hyperemia. How far have we advanced in understanding the pathogenesis of migraine?
RC: The pathophysiology of migraine has changed dramatically over the last 2 decades. Today migraine is understood as a neurological disease with a genetic predisposition. Sufferers inherit a nervous system that is more vigilant of its surroundings than the brain of a non-migraineur, and this nervous system has an enduring predisposition to recurrent attacks of migraine triggered by events that do not produce migraine in the general population. This tendency spans decades of life for most migraineurs. Migraine is the quintessential example of how the genetic makeup of the individual and their environment can interact to produce an attack of migraine and over time the disease of migraine.
An attack of migraine occurs when the nervous system encounters triggering events that overwhelm the brain’s capacity to adjust. The first phase of a migraine is called the premonitory period or prodrome. This period is characterized by non-headache symptoms such as fatigue, cognitive change, sensory sensitivity, nasal congestion, muscle pain, yawning. This can be a warning for many people that an attack of disabling migraine is inevitable.
The second phase is called the aura and occurs in approximately 30% of attacks. This represents an electrical event in the brain called spreading cortical depression and produces a period of neurological changes that can last up to one hour but the symptoms are fully reversible. Symptoms generally are visual such as flashing lights or sensory such as numbness in the face or upper extremity.
The third phase is the headache phase. It usually begins with a mild headache that progresses sometimes very rapidly into a moderate to severe headache that is associated with nausea, sometimes vomiting and sensory sensitivity to light, sound, touch, and smell. Also there is frequently muscle pain in the head, neck, and shoulders and nasal congestion or “sinus” symptoms. However, large studies consistently show that what most physicians or patients consider sinus headache is actually migraine. This generally causes a person to seek refuge in a dark quiet place and generally lasts from 4-72 hours.
The final phase is called the postdrome. Sometimes it is referred to as the migraine hangover and consists of muscle aches and pain, slowed cognition, fatigue, and general malaise that can last up to another 24 hours. More rarely, some people experience a boost in energy and elation.
Read the whole thing here
06 June 2009
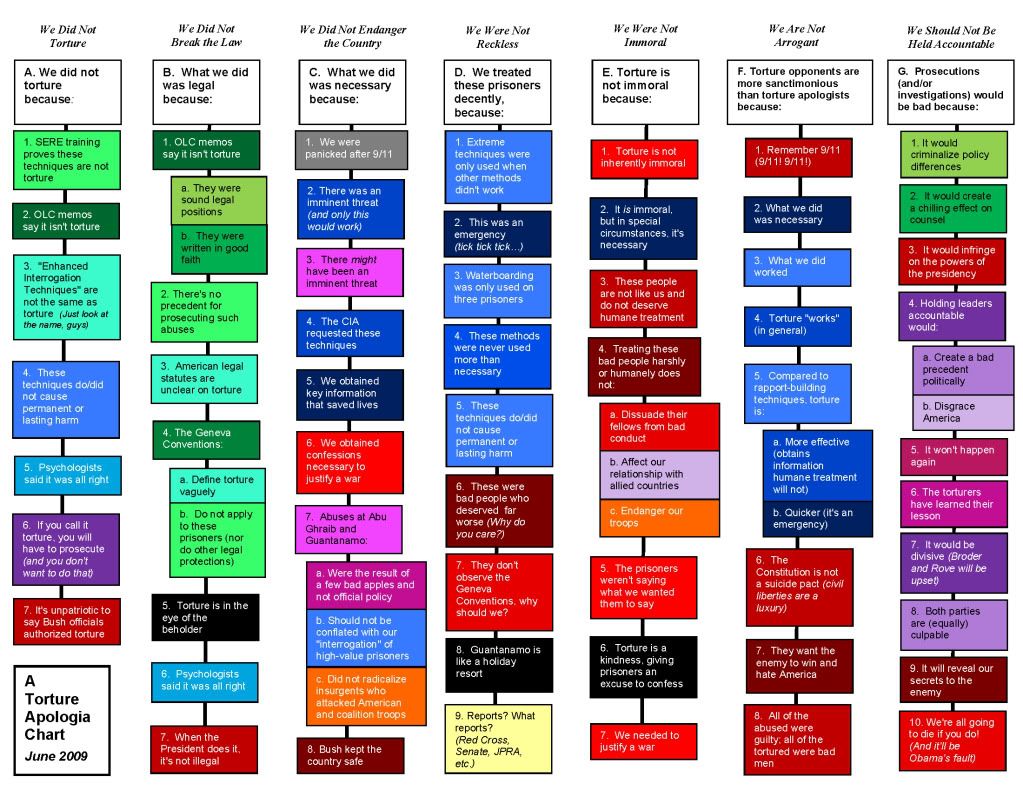
Guide to torture justifications
Having trouble keeping up with the lines of justification for the US torture regime? Digby brings you a handy chart:

Go here for a larger version.
Go here for a larger version.
Subscribe to:
Posts (Atom)

{kind=link}