Okay. In the last post I mentioned that I get annoyed when concerns about opioids being diverted pop up in discussions about when opioids are indicated treatments. It's not that I don't think diversion is an important concern in drug policy. It's just that I feel like it shouldn't be part of discussions of when opioids are good treatments.
Anyway, I was annoyed by not knowing I feel this way.* So, the following is some off-the-cuff noodling about when concerns are relevant in decisions about the use of opioid drugs. I'm not at all sure about how much of it I want to stand behind. But hopefully it might be useful for sparking some discussion.
*I remember someone once telling me that philosophy starts with a sense of wonder. I have since found that, for me, it usually starts with annoyance; it ends in wonder.
-------------
In general, I tend to think that the dangers of opioid diversion --opioids ending up outside of the patient's hands-- get too much weight in discussions of drug policy (although some recent statistics on overdose and death rates involving opioids are giving me some pause in my beliefs about the severity of diversion's harms).
But in addition to questions about how severe the consequences of diversion are, we also need to know whose problem it is. A comprehensive drug policy spans many different areas including, inter alia, the law in its criminal, civil, and regulatory forms; professional determinations of best clinical practices; and individual clinicians' decisions about how to treat individual patients. Thus we need to know whether preventing diversion should have the same importance for everyone involved in the prescription drug arena.
I'm going to suggest that preventing diversion can be a legitimate concern at the more general levels. And they may inform doctors practices in a general way. But, I suspect, the potential harms resulting from diversion should not factor into a doctor's decisions about what medications to prescribe a patient.
My claims here will rest on the supposition that a clinician's ethical responsibilities arise from her patient's individual welfare. Her professional obligation is not the promotion of the general welfare via her interactions with a certain individual. The clinician's responsibility is to alleviate her patient's suffering in the safest and most effective way available.
A rough analogy may help bring out this distinction between duties based in the promotion of the general welfare and duties based in the promotion of an individual's welfare. In an adversarial system of criminal justice like we have in the United States, the role of a defense attorney is to advocate for her clients interests as best she can. Even if she recognized that her client's conviction may benefit the public at large, she is obligated to ignore that fact in doing her job. This doesn't mean that the job of defense attorney is entirely removed from the enterprise of promoting the public good. It's that a system in which a party is assigned to look out only for the interests of the defendant is more likely to be better overall. (One major disanalogy here is that my supposition about the source of the doctor's duties need not appeal to claims about what would best promote the general welfare.)
If we a clinician's duties as tied her patient's welfare in this way, concerns about the welfare of others are thus (nearly always) irrelevant to decisions about what substances to prescribe her patient. This suggests that even though the clinician may foresee that others may be harmed through diversion if she prescribes an opioid to a patient, this possibility should have no weight in her decision about what to prescribe. Her duty arises from and is directed at the health of her patients, not the health of people in general.
Obviously, this has its limits. Massive harms to others may trump this obligation. And it may be that if two treatments were exactly equal in their efficacy and safety, then considerations of the general good or other effects on others may break the tie.
Nor does this mean that the doctor must completely ignore the possibility that the drug will be diverted. Other public entities' interests in preventing diversion are based in their obligation to protect public health overall. But given the source of her professional obligations, the clinician's concerns about diversion should be limited to its effects on her patient's health.
Clearly, a responsible clinician must be attuned to the possibility that the patient herself will divert the drug. But her vigilance is not demanded by the need to prevent harms to the recipients of the diversion. It comes from her responsibilities to the patient. The clinician's treatment decisions must be based on the supposition that the patient will comply with the prescribed regime. She cannot aim to promote an individual's welfare by prescribing her a substance that she believes that the patient will not take. Therefore, the belief that the patient will take the drug as prescribed is a necessary condition of justifiably prescribing an opioid.
Suppose that a patient is accompanied by a stoned adolescent whose T-shirt reads "I love drugs!" Does this necessary condition imply that she ought to take into consideration the likelihood that the son will divert the drugs?
The answer seems to be yes. She cannot prescribe a medication to benefit her patient if she believes that the patient won't take the drug because someone else will steal it. Of course, it's unlikely that the suspicion in this case would justify her refusing to prescribe an otherwise indicated opioid Much will hang on the strength of her conviction that the drug will be diverted. In the drug diverting adolescent case, the clinician may be required to put special emphasis on the need to keep control of the medication in counseling the patient. But as long as she can be satisfied that the patient will be reasonably vigilant, she will be justified in writing the prescription. Her uncertainty about the likelihood of diversion combined with the need to respect the patient's autonomy will set the bar for reasonable vigilance pretty low.
Cases in which she should altogether refuse to prescribe on these grounds will likely be rare. But they are easy to imagine. Suppose that a disabled patient is completely dependent on her caretaker for all of her medications. If the clinician was convinced that the caretaker would divert a significant portion of the prescribed opioid, then she should not write the prescription. Indeed, doing so would be tantamount to writing the prescription for the caretaker. Though, she may have some obligation to seek other ways of getting the indicated treatment to the patient (e.g., recommending at home nursing visits, and patient treatment).
What's important is the way concerns about diversion are figuring in here. A clinician should be cautious of diversion insofar as it would interfere with her patient's treatment. Her responsibilities do not depend on how the recipients of the diverted substance may be affected. Those dangers of diversion give her reason to, for example, keep her cabinets locked. But they should be irrelevant to her decisions about patients' treatments.
This is not to say that a comprehensive drug policy should not be concerned about the harms to non-patients who gain access to opioids through diversion. It is a fact that the availability of opioids in legitimate channels will involve some diversion and some non- patients will be harmed. While the clinician's responsibility is based in her individual patient's welfare, government policies are properly attuned to protecting welfare across the board. Thus entities (in the US) like the FDA, the Department of Justice and the DEA are justified in creating policies and enforcement practices which will minimize the amount of diversion.
But this picture of the clinician's obligations does create tension between the government's proper aims creating drug policy and the duties of clinicians. We should thus want a principled way of resolving these kinds of inevitable conflict. One possibility is that one set of considerations will always trump the other (that is, the first set is lexically prior to the other).
To see the implications of a lexical ordering of these considerations suppose that the paramount consideration in shaping drug policy was ensuring clinicians' abilities to carry out their duties to their patients. This would have implications for how we decide conflicts. Such a partial lexical ordering would entail that the protection of access to safe and effective drugs cannot be trumped by considerations about diversion. More generally, this might mean that any proposed policy that would promote the general good could be vetoed if it unreasonably affected the ability of clinicians to treat their patients.
This ordering of concerns would be unlikely to undermine reasonable restrictions on the use and prescription of opioids. For example, this is compatible with a well regulated and organized system for inventory control in the manufacturing, shipping, and distribution of opioids. The same is true for methods of verifying the legitimacy of prescriptions and the identity of patients. But some apparently relatively mild restrictions on prescribing ability may not be compatible with this set of drug policy priorities.
For example, the FDA is presently considering requiring all clinicians who prescribe powerful long-acting opioids to have a special certification. Many general practice clinicians who currently prescribe such medications may be unwilling to go through the hassle of obtaining and maintaining the certification. If the certification process was unduly difficult, many clinicians would be unable to prescribe the medications that they thought were best indicated for their patients conditions. Such a regulation would likely decrease the number of deaths from diversion. But no matter how many diversion related deaths would be prevented, it should be rejected if we believe that the clinician's abilities to treat their patients should always trump any other consideration.
So, in sum, here's what I've suggested: If we think about the source and nature of clinicians' professional obligations in a particular way, then concerns about diversion should not play a role in determining whether to prescribe an opioid (outside of diversion undermining the treatment regime). Direct focus on preventing diversion is instead the job of regulatory agencies whose mission is the common public good.
I haven't given any argument in favor of the further idea that concerns about diversion should always be subordinated to clinicians ability to prescribe opioids as they see fit. Though I am definitely attracted to this view. We can leave that a subject for another post.
25 June 2009
Opioids often preferable to NSAID's in the elderly
This is important.
The NYT reports that in light of findings that
The American Geriatrics Society
Editorial comment: I'm unhappy that the reporter chose to use this quote in emphasizing that opioids have their own dangers:
Diversion of opioids is a real problem. But it really annoys me to see it used as a counterpoint in discussions of their clinical usefulness.
I almost feel like these claims are saying something like: Advil might kill Grandma, but we might not want to give her a safer treatment because her grandson might steal it and kill himself.' (I don't think the reporter or Dr. Chou intended it this way --that's just how I take it)
Update: I was bothered by not knowing why the stuff about diversion annoys me so much. So I've posted some very rough thoughts here.
The NYT reports that in light of findings that
[in elderly patients] The risks of Nsaids include ulcers and gastrointestinal bleeding and, with some drugs, an increased risk of heart attacks or strokes. The drugs do not interact well with medicines for heart failure and other conditions, and may increase high blood pressure and affect kidney function, experts said.
The American Geriatrics Society
removed those everyday medicines, called Nsaids, for nonsteroidal anti-inflammatory drugs, from the list of drugs recommended for frail elderly adults with persistent pain. The panel said the painkillers should be used “rarely” in that population, “with extreme caution” and only in “highly selected individuals.”
[....]
“We’ve come out a little strong at this point in time about the risks of Nsaids in older people,” said Dr. Bruce Ferrell, a professor of geriatrics at U.C.L.A. who is chairman of the panel. “We hate to throw the baby out with the bathwater — they do work for some people — but it is fairly high risk when these drugs are given in moderate to high doses, especially when given over time.
“It looks like patients would be safer on opioids than on high doses of Nsaids for long periods of time,” he continued
Link (My italics; I've interpolated the order of the paragraphs)
Editorial comment: I'm unhappy that the reporter chose to use this quote in emphasizing that opioids have their own dangers:
“We’re seeing huge increases nationwide of reports about the misuse and diversion of prescription drugs and related deaths,” said Dr. Roger Chou, a pain expert who was not involved in writing the guidelines for the elderly but directed the clinical guidelines program for the American Pain Society. “The concerns about opioids are very real.”
Diversion of opioids is a real problem. But it really annoys me to see it used as a counterpoint in discussions of their clinical usefulness.
I almost feel like these claims are saying something like: Advil might kill Grandma, but we might not want to give her a safer treatment because her grandson might steal it and kill himself.' (I don't think the reporter or Dr. Chou intended it this way --that's just how I take it)
Update: I was bothered by not knowing why the stuff about diversion annoys me so much. So I've posted some very rough thoughts here.
16 June 2009
Resources for Causalgia (CRPS/RSD)
Here's a helpful guide to resources on Complex Regional Pain Syndrome/Reflex Sympathetic Dystrophy (CRPS/RSD/Causalgia)
For those of you who don't know, Causalgia (CRPS/RSD) should rank high on the list of 'Things-You-Don't-Want'.
On the IASP definition:
Or as it was first described by Silas Weir Mitchell in 1872 after the Civil War
In other words, in causalgia part of your body feels like it's constantly on fire.
Resources and Relief for Reflex Sympathetic Dystrophy
For those of you who don't know, Causalgia (CRPS/RSD) should rank high on the list of 'Things-You-Don't-Want'.
On the IASP definition:
Causalgia
A syndrome of sustained burning pain, allodynia, and hyperpathia after a traumatic nerve lesion, often combined with vasomotor and sudomotor dysfunction and later trophic changes.
Or as it was first described by Silas Weir Mitchell in 1872 after the Civil War
"We have some doubt as to whether this form of pain ever originates at the moment of the wounding. . . Of the special cause which provokes it, we know nothing, except that it has sometimes followed the transfer of pathological changes from a wounded nerve to unwounded nerves, and has then been felt in their distribution, so that we do not need a direct wound to bring it about. The seat of the burning pain is very various; but it never attacks the trunk, rarely the arm or thigh, and not often the forearm or leg. Its favorite site is the foot or hand. . . Its intensity varies from the most trivial burning to a state of torture, which can hardly be credited, but reacts on the whole economy, until the general health is seriously affected....The part itself is not alone subject to an intense burning sensation, but becomes exquisitely hyperanesthetic, so that a touch or tap of the finger increases the pain." quoted in UCLA pain exhibit
In other words, in causalgia part of your body feels like it's constantly on fire.
Online introduction to pain processes
The-New-Science-of-Pain-Relief has a nice introductory walkthrough of the basic neurology of pain here.
Philosophers will, of course, carefully take note the role of C nociceptive afferents.
Philosophers will, of course, carefully take note the role of C nociceptive afferents.
11 June 2009
ABC story on FDA Acetaminophen overdose report
With every changing of the seasons comes a new set of cautions about acetaminophen use.
Like the changing of the leaves, experts call for better public education and packaging practices.
And, like the migration of the butterflies^, the pharmaceutical industry tells them to go f*** themselves:
See this show again in a few months and a couple thousand more deaths.
^Sorry for the bad simile
Like the changing of the leaves, experts call for better public education and packaging practices.
And, like the migration of the butterflies^, the pharmaceutical industry tells them to go f*** themselves:
McNeil Consumer Healthcare, a Johnson & Johnson subsidiary and the manufacturer of Tylenol, said in a statement Thursday that they fear the [FDA report's] recommendations could have the effect of steering consumers away from an appropriate and safe drug.
"While we share the FDA's mutual goal of preventing and decreasing the misuse and overdose of acetaminophen, we have concerns that some of the FDA recommendations could discourage appropriate use and are not necessary to addressing the root causes of acetaminophen overdose," the statement reads. Link
See this show again in a few months and a couple thousand more deaths.
^Sorry for the bad simile
Pain in animal slaughter
Newsflash!
Cutting calves throats hurts, study says...
Cutting calves throats hurts, study says...
N Z Vet J. 2009 Apr; 57(2): 74-6
Mellor DJ, Gibson TJ, Johnson CBCommercial slaughter of farm livestock usually employs an extensive incision that severs the soft tissues of the neck including the major blood vessels supplying and draining the brain. It is intended to cause a catastrophic decrease in cerebral blood flow with rapid onset of unconsciousness or insensibility. The tissues of the neck are innervated with nociceptive nerve fibres and their transection will cause a barrage of sensory impulses. Consciousness, and therefore the ability of the animal to feel pain and experience distress after the incision, may persist for 60 seconds or longer in cattle. These observations suggest that livestock may experience pain and distress during the period before they become unconscious (insensible). Psychological shock and fear may also be associated with the extensive tissue damage and blood loss. Pre-incision stunning has been adopted as a precautionary measure to prevent suffering. However, the question remains: How intense and noxious are these experiences? Recent methodological developments related to quantitative analysis of the electroencephalogram (EEG) allow the experience of pain to be assessed more directly than has hitherto been possible. This methodology has now been applied to the question of the slaughter of calves by ventral-neck incision. The new information demonstrates clearly for the first time that the act of slaughter by ventral-neck incision is associated with noxious stimulation that would be expected to be perceived as painful in the period between the incision and loss of consciousness. These data provide further support for the value of stunning in preventing pain and distress in animals subjected to this procedure."
(Via HubMed - pain.)
Obstetric anesthesia: Past present and future.
And yet another addition to my never ending reading list.
Obstetric anesthesia: Past present and future.: "
J Matern Fetal Neonatal Med. 2009 Jun 1; 1-4
Kuczkowski KMObstetric anesthesia is science and art combined, and obstetric anesthesiologists must be concerned simultaneously with the lives of (at least two) intricately interwoven patients - the mother and her baby (ies). Obstetric anesthesia, by definition, is a subspecialty of anesthesia devoted to peripartum, perioperatvie, pain and anesthetic management of women during pregnancy and the puerperium. Perhaps no other subspecialty of anesthesiology provides more personal gratification than the practice of obstetric anesthesia. An obstetric anesthesiologist has become an essential member of the peripartum care team, who closely works with the obstetrician, perinatologist, midwife, neonatologist and labor and delivery nurse to ensure the highest quality care for the pregnant woman and her baby. Exchange on information and communication skills in ever changing environment of labor and delivery is essential for perfect outcome, which is always expected when providing safe passage for both the mother and her fetus from antepartum to postpartum period. Changes in maternal-fetal and neonatal medicine and obstetric anesthesia have continued to develop rapidly during the recent years. The purpose of this article is to explore a number of important issues in modern practice of obstetric anesthesia."
(Via HubMed - pain.)
Effect of mental stress on cold pain in chronic tension-type headache sufferers.
Here's a little bit about headache and stress.
Effect of mental stress on cold pain in chronic tension-type headache sufferers.: "
J Headache Pain. 2009 Jun 5;
Cathcart S, Winefield AH, Lushington K, Rolan PMental stress is a noted contributing factor in chronic tension-type headache (CTH), however the mechanisms underlying this are not clearly understood. One proposition is that stress aggravates already increased pain sensitivity in CTH sufferers. This hypothesis could be partially tested by examining effects of mental stress on threshold and supra-threshold experimental pain processing in CTH sufferers. Such studies have not been reported to date. The present study measured pain detection and tolerance thresholds and ratings of supra-threshold pain stimulation from cold pressor test in CTH sufferers (CTH-S) and healthy Control (CNT) subjects exposed to a 60-min stressful mental task, and in CTH sufferers exposed to a 60-min neutral condition (CTH-N). Headache sufferers had lower pain tolerance thresholds and increased pain intensity ratings compared to controls. Pain detection and tolerance thresholds decreased and pain intensity ratings increased during the stress task, with a greater reduction in pain detection threshold and increase in pain intensity ratings in the CTH-S compared to CNT group. The results support the hypothesis that mental stress contributes to CTH through aggravating already increased pain sensitivity in CTH sufferers."
(Via HubMed - pain.)
Acupuncture And Pain
In answer to a reader's question, How To Cope With Pain digs up some conclusions about the efficacy of acupuncture.
Acupuncture And Pain: "An excellent review article by Edzard Ernst, M.D., reports that the conditions that are most solidly backed up by evidence showing acupuncture helps are:
- chemotherapy-induced nausea/vomiting
- postoperative nausea/vomiting
- idiopathic headache (headache of unknown cause)
Many other diseases, both pain-related and not, were not helped by acupuncture. Ernst concludes that studies ‘do not suggest that this treatment is effective for a wide range of conditions.’"
[Read the rest for some limitations in the current literature]
The original article is Acupuncture: What does the most reliable evidence tell us?, in the Journal of Pain and Symptom Management 2009, Vol 37, pages 709-714.
(Via How To Cope With Pain Blog.)
Palliative care for a patient with anorexia nervosa
Pallimed brings up a very hard case. I'm honestly not sure what I think about much of this:
Palliative care & eating disorders: "The International Journal of Eating Disorders has a case report and discussion of a patient with refractory anorexia nervosa who died receiving hospice care. This is one fascinating case report. The case, to summarize briefly, involved a young woman with a long history of anorexia nervosa, refractory to all attempts at treatment (including involuntary/forced treatment) who apparently also was not deemed a candidate for forced guardianship (the hospital's legal counsel advised she would not meet requirements to be declared incompetent).
This is how they describe the ethics committee's response to the case:The committee’s members struggled to understand how one could die from a psychiatric illness (other than by suicide or unintentional overdose) and were not sure how to proceed. Although they could delineate the differences between acute mental health risks such as suicide, drug overdoses, psychosis or self-neglect, they had no points of reference regarding how to manage a patient who was chronically a danger to herself, unwilling to engage in further treatments, and unresponsive to all prior attempts to treat her involuntarily. The only examples the committee raised for comparison concerned drug users who received heart valve replacements, yet continued to use, knowing that such ongoing use would kill them. In such cases, if a high risk of ongoing subsequent IV drug use was suspected ahead of time, the decision was often made not to provide valve replacements, but there was no forced treatment.This is how they presented what palliative care for anorexia nervosa would look like to the patient (italics mine):If she chose to pursue treatment she would be assisted, but the staff would not force her into any involuntary placements or impose any treatment she did not want. There would be no weigh-ins, no calorie or exercise monitoring, no IM medications and no required therapy sessions. She would be offered outpatient therapy only as she felt desirable and necessary. Psychiatric medications would be prescribed as the patient deemed necessary to help manage depression, anxiety and insomnia. The patient would receive weekly visits from a palliative care nurse, who would work with her to manage her symptoms and keep her comfortable. The patient agreed to no further hospitalizations, but did not fully agree with the plan for ‘‘palliative care’’ since she did not believe she was going to die.The patient basically continued her illness behaviors, got weaker/sicker, and was eventually enrolled in an inpatient hospice where she died.
Some observations.
- AN is clearly at times a terminal illness, refractory to all attempts to reverse it.
- In this case it was clear that the patient's life could have been prolonged although only with forced treatment. It was the opinion of her physicians that such forced treatment, while life-prolonging, would not 'cure' her AN (for some patients a trial, or many trials, of forced nutritional treatment along with psychiatric care gets them to the point at which they are willing to continue with voluntary treatment and can have a durable response; it was felt this would never happen with this patient). Thus the decision came down to trying to force further involuntary treatment vs. letting the disease run its natural course with her inevitably dying.
- I found it interesting that they did not feel there was enough of a chance she'd be considered incompetent that they didn't even put her through the court process. Her statement that she did not think she would die (and it seems she continued that belief until the end, and persisted at least until she was enrolled in hospice in saying that she in fact wanted to live) seems to me to indicate such a fundamental lack of insight into her condition that I'm not sure I believe that. Granted, I'm not too familiar with criteria for declaring someone incompetent on psychiatric grounds, but I assume it has something to do with one's mental illness being such that one cannot even take in basic medical information.
- That said, and even if she was legally stripped of her decision-making rights, for situations in which even involuntary treatment would not work long-term, is it right to force patients to do that? In this situation they concluded No, and made plans accordingly, which seemed to work as well as could be expected under the circumstances.
[A very interesting discussion follows in the rest. Definitely give it a read]
Treating Psychiatric Symptoms
From the How To Cope With Pain Blog, here's a bit about the role of a psychiatrist in comprehensive pain management:
Treating Psychiatric Symptoms: "
Welcome to the continuing series Why You Should See a Pain Management Psychiatrist. Last week we learned that psychiatric symptoms - such as depression, anxiety, etc. - often accompany chronic pain. This week we’ll look at how to treat psychiatric diseases.
As we saw, depression (8-50% of patients with pain), anxiety (19-50%), PTSD (10%), sleep disturbance (50% or more), drug and alcohol problems (3-19%) are common in patients with pain. Let’s look at some important issues related to treating these problems.
1. Identifying symptoms
To be able to treat psychiatric symptoms, they first have to be identified. Your doctor should be asking about these common symptoms and referring you if appropriate. You should also report if you’re having such symptoms. Don’t be embarrassed or feel like you’re complaining. Getting help is important!
2. Taking symptoms seriously
If you’re having significant depression, anxiety or other symptoms, it’s important to report these to start to get treatment for them. These symptoms should not be dismissed as, ‘of course you have depression - it’s because of your pain.’ Chronic pain does not automatically mean depression, anxiety and disturbed sleep. There’s treatment for these symptoms.! And they should be treated!
3. Treat all the disorders that are present.
We know that if psychiatric problems are present along with pain, it’s crucial to treat both. Treating just 1 doesn’t make the other go away. For example, if someone has depression and pain, treating just pain doesn’t necessarily mean the depression will go away. And sometimes neither gets better unless you treat both.
4. Treatment
There are both therapies and medications to treat nearly all psychiatric diseases. Medication should be used only along with therapy. I strongly recommend trying therapy first, before medication, to see if just therapy alone can work. There are times, when psychiatric symptoms are severe, that both will be started at once, but that’s less common. Most people with pain disorders are already on several medications and sometimes already tolerating side effects, so trying non-medication treatment first makes sense.
Other articles in the series:
"
- Why comprehensive treatment works better
- Benefits of a psychiatric evaluation
- Treatment of psychiatric symptoms
- Using psychiatric medications for pain
- Learning psychological skills
- Making positive behavioral changes
- Making positive psychological changes
- Benefits of supportive therapy
- Benefits of a pain support group
- New brain-based treatments
(Via How To Cope With Pain Blog.)
Refusal to torture in Milgram experiments
Oh well. From Brain Blogger, a new experiment which deflates some of the hope for humanity I had held out in the face of the Milgram experiments on torture and obedience to authority:
Though I think Dr. Surve is reaching quite a bit in concluding that
The first sentence gets some support from the experiment. I don't see why the second would.
Not that that's much consolation.
For the first time in over 30 years, a scientist named Dr. Jerry Burger managed to obtain approval for a study partially reproducing the Milgram experiment, and in 2009 he published his findings in the journal American Psychologist....Dr. Burger also had some subjects witness a planted tester who refused to administer the test. He hypothesized that seeing a prior refusal might embolden test subjects to also refuse. Nevertheless, Dr. Burger’s results were comparable to Dr. Milgram’s results, and having a witnessed refusal did not significantly change [the willingness of subjects to continue increasing the voltage of the shocks].
References
Burger, J. (2009). Replicating Milgram: Would people still obey today? American Psychologist, 64 (1), 1-11 DOI: 10.1037/a0010932
Though I think Dr. Surve is reaching quite a bit in concluding that
Whatever moral compass human beings claim to possess, this research suggests that when presented with a perceived authority figure, the majority will override that compass in favor of obedience. The only possible conclusion, then, is that most human beings are in fact hard-wired to torture.
The first sentence gets some support from the experiment. I don't see why the second would.
Not that that's much consolation.
Sphenopalatine ganglioneuralgia (aka Brain Freeze)
Brain Blogger has a primer here.
It's based on this article:
Kaczorowski, M. (2002). Ice cream evoked headaches (ICE-H) study: randomised trial of accelerated versus cautious ice cream eating regimen. BMJ, 325(7378), 1445-1446. DOI: 10.1136/bmj.325.7378.1445
Sigh. I must be in the wrong field. Not much ice cream related research in philosophy.
It's based on this article:
Kaczorowski, M. (2002). Ice cream evoked headaches (ICE-H) study: randomised trial of accelerated versus cautious ice cream eating regimen. BMJ, 325(7378), 1445-1446. DOI: 10.1136/bmj.325.7378.1445
Sigh. I must be in the wrong field. Not much ice cream related research in philosophy.
Migraines
From Brain Blogger Dr. Shaheen Lakhan's interview with headache expert Dr. Roger K Cady, a bit about the current understanding of what migraines are:
Read the whole thing here
Shaheen Lakhan: To start off, what sets a migraine apart from a tension-type headache?
Roger Cody: ...tension headache is a headache without the presence of other symptoms. The headache is generally mild to moderate in intensity, more likely to be on both sides of the head and with a steady and pressure quality to the pain. It is not associated with nausea or sensitivity to light or sound.
Migraine is the most common headache causing people to seek medical attention. Migraine is always more than just a headache. The headache can be on one or both sides of the head and more likely to have a throbbing quality or to be made worse by daily activity or things like bending over. Associated with the headache are symptoms like nausea and sensitivity to light, sound, and other sensory stimuli.
[....]
In people with migraine, many experts suggest that migraine and tension headaches exist on the same spectrum and arise out of the same pathophysiological process (big and little migraines).
SL: I recall the vascular theory of migraine from decades past which held that migraine symptoms were a function of ischemia and hyperemia. How far have we advanced in understanding the pathogenesis of migraine?
RC: The pathophysiology of migraine has changed dramatically over the last 2 decades. Today migraine is understood as a neurological disease with a genetic predisposition. Sufferers inherit a nervous system that is more vigilant of its surroundings than the brain of a non-migraineur, and this nervous system has an enduring predisposition to recurrent attacks of migraine triggered by events that do not produce migraine in the general population. This tendency spans decades of life for most migraineurs. Migraine is the quintessential example of how the genetic makeup of the individual and their environment can interact to produce an attack of migraine and over time the disease of migraine.
An attack of migraine occurs when the nervous system encounters triggering events that overwhelm the brain’s capacity to adjust. The first phase of a migraine is called the premonitory period or prodrome. This period is characterized by non-headache symptoms such as fatigue, cognitive change, sensory sensitivity, nasal congestion, muscle pain, yawning. This can be a warning for many people that an attack of disabling migraine is inevitable.
The second phase is called the aura and occurs in approximately 30% of attacks. This represents an electrical event in the brain called spreading cortical depression and produces a period of neurological changes that can last up to one hour but the symptoms are fully reversible. Symptoms generally are visual such as flashing lights or sensory such as numbness in the face or upper extremity.
The third phase is the headache phase. It usually begins with a mild headache that progresses sometimes very rapidly into a moderate to severe headache that is associated with nausea, sometimes vomiting and sensory sensitivity to light, sound, touch, and smell. Also there is frequently muscle pain in the head, neck, and shoulders and nasal congestion or “sinus” symptoms. However, large studies consistently show that what most physicians or patients consider sinus headache is actually migraine. This generally causes a person to seek refuge in a dark quiet place and generally lasts from 4-72 hours.
The final phase is called the postdrome. Sometimes it is referred to as the migraine hangover and consists of muscle aches and pain, slowed cognition, fatigue, and general malaise that can last up to another 24 hours. More rarely, some people experience a boost in energy and elation.
Read the whole thing here
06 June 2009
Guide to torture justifications
Having trouble keeping up with the lines of justification for the US torture regime? Digby brings you a handy chart:

Go here for a larger version.
Go here for a larger version.
14 May 2009
Israeli GSS cases
http://www.jafi.org.il/education/actual/gss.html
http://www.mfa.gov.il/MFA/Government/Law/Legal%20Issues%20and%20Rulings/Supreme%20Court%20Judgment%20Concerning%20the%20Legality%20of
http://elyon1.court.gov.il/files_eng/94/000/051/a09/94051000.a09.HTM
http://www.mfa.gov.il/MFA/Government/Law/Legal%20Issues%20and%20Rulings/Supreme%20Court%20Judgment%20Concerning%20the%20Legality%20of
http://elyon1.court.gov.il/files_eng/94/000/051/a09/94051000.a09.HTM
06 May 2009
The day after the day after
Question: When I haven't been to judo in a few weeks, I'm more sore 48 hours after practice than I am 24 hours afterward. But after getting back in shape the soreness seems to constantly decrease with time. Other people tell me similar things with other new exercise regimes. So I don't think I'm idiosyncratic. Why does this happen?
My initial thought --and here I reveal the depth of my ignorance-- was that since the tissues have been healing, the worsening allodynia isn't due to increased prostaglandins, bradykinin, leukotrienes, etc, released by the damaged muscle. Rather it's from dorsal horn wind-up, and neurogenic inflammatory factors like substance p and neurokinins A and B. It makes sense that those would continue to increase over time.
But that wouldn't explain why this doesn't seem to happen when I'm already in shape, even when a workout is much harder than usual.
Or is it just the obvious answer that the difference between relative inactivity and a moderate workout is less than the difference between a moderate workout and a really hard one?
Ideas?
My initial thought --and here I reveal the depth of my ignorance-- was that since the tissues have been healing, the worsening allodynia isn't due to increased prostaglandins, bradykinin, leukotrienes, etc, released by the damaged muscle. Rather it's from dorsal horn wind-up, and neurogenic inflammatory factors like substance p and neurokinins A and B. It makes sense that those would continue to increase over time.
But that wouldn't explain why this doesn't seem to happen when I'm already in shape, even when a workout is much harder than usual.
Or is it just the obvious answer that the difference between relative inactivity and a moderate workout is less than the difference between a moderate workout and a really hard one?
Ideas?
05 May 2009
Regional blocks better for Cesarean sections
Medical News Today
For Cesarean Section, Regional Blocks Prove Superior To General Anesthesia
30 Apr 2009
General anesthesia (GA) is associated with an increased risk of infant intubation and low Apgar scores, relative to regional anesthesia. An analysis of 50,806 cesarean deliveries, published in the open access journal BMC Medicine, strongly supports guidelines that regional anesthesia is to be preferred over GA for most cesarean sections.
Charles Algert, from the Kolling Institute at the Royal North Shore Hospital, Sydney, was part of a team of researchers who studied births in the state of New South Wales, Australia, between 1998 and 2004. He said, "We have shown that general anesthesia poses significant risks to the neonate of both resuscitation requiring intubation and of a poor Apgar score at 5 minutes. The greatest relative risk of both adverse outcomes occurred in low-risk, planned, repeat cesarean deliveries under GA, but the greatest excess in risk attributable to GA was for emergency deliveries for fetal distress where the infant would already have been compromised to some extent".
Although current guidelines recommend regional blocks, GA was still used for 12.6% of cesareans across NSW in 2006. According to the NHS Maternity Statistics, 8.7% of cesarean sections in England in 2006-2007 were performed using GA. It is generally presumed that any harm caused by GA is short-lasting, with most studies focusing on resuscitation and the Apgar score at one minute. According to Algert, however, this may not be the case, "The increased rates of neonatal intubation after GA shown in this study represent harm in and of itself, and the persistence of low 5-minute Apgar scores suggests that deleterious effects may last longer than the immediate aftermath of delivery".
The authors conclude, "Clinicians considering the use of GA for a cesarean delivery should be aware of these possible consequences for the infant, for both planned and emergency sections".
Regional block versus general anaesthesia for caesarean section and neonatal outcomes: a population-based study
Charles S Algert, Jennifer R Bowen, Warwick B Giles, Greg E Knoblanche, Samantha L Lain and Christine L Roberts
BMC Medicine (in press)
Article available at journal website: http://www.biomedcentral.com/bmcmed/
Source:
Graeme Baldwin
BioMed Central
Article URL: http://www.medicalnewstoday.com/articles/148091.php
02 May 2009
New warning labels on NASIDs
Medical News Today News Article: "FDA Requires Additional Labeling For Over-the-Counter Pain Relievers And Fever Reducers To Help Consumers Use Products Safely
29 Apr 2009
The Food and Drug Administration issued a final rule today that requires manufacturers of over-the-counter (OTC) pain relievers and fever reducers to revise their labeling to include warnings about potential safety risks, such as internal bleeding and liver damage, associated with the use of these popular drugs.
Products covered by the FDA action include acetaminophen, and a class of drugs known as the nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs include aspirin, ibuprofen, naproxen, and ketoprofen. Acetaminophen is in a class by itself. The revised labeling applies to all OTC pain relievers and fever reducers, including those that contain one of these ingredients in combination with other ingredients, such as in cold medicines containing pain relievers or fever reducers.
'Acetaminophen and NSAIDs are commonly used drugs for both children and adults because they are effective in reducing fevers and relieving minor aches and pain, such as headaches and muscle aches, ' said Charles Ganley, M.D., director, FDA's Office of Nonprescription Drugs in the Center for Drug Evaluation and Research. 'However, the risks associated with their use, need to be clearly identified on the label so that consumers taking these drugs are fully aware of the potential harm they can cause. It is important that they know how to take these medications safely to reduce their risk.'
Under the final rule, manufacturers must ensure that the active ingredients of these drugs are prominently displayed on the drug labels on both the packages and bottles. The labeling also must warn of the risks of stomach bleeding for NSAIDs and severe liver damage for acetaminophen.
Since 2006, some manufacturers have voluntarily revised their product labeling to identify these potential safety concerns. However, the voluntary changes to labeling do not address all of the labeling requirements in the new rule. For example, the new rule includes a warning on products containing acetaminophen that instructs consumers to ask a doctor before they are taking the blood thinning drug warfarin. The new rule requires all manufacturers to relabel their products within one year of today's date.
Safety data reported in medical literature indicate that people sometimes take more acetaminophen than the labeling recommends. Others unknowingly take multiple products containing acetaminophen at the same time. Exceeding the recommended dosage of acetaminophen may increase the risks for severe liver damage. Alcohol use can also increase the risk of liver damage with acetaminophen.
The risk for stomach bleeding may increase in people who use NSAIDs and who are taking blood-thinning drugs (anticoagulants) or steroids. Stomach bleeding risks also increase for people who take multiple NSAIDs at the same time, or in people who take them longer than directed. Alcohol use can increase the risk for stomach bleeding with NSAIDs use.
An FDA Advisory Committee meeting will be convened on June 29 & 30, 2009, to discuss further steps the FDA could take to reduce the risk of liver damage associated with acetaminophen overdoses.
To read the final rule on the relabeling of OTC pain relievers and fever reducers, go here.
To read the FR Notice announcing the FDA Advisory Committee meeting, see link.
Source
Food and Drug Administration
Article URL: http://www.medicalnewstoday.com/articles/148085.php"
Medical News Today News Article
Medical News Today News Article: "Stroking The Skin Sends Signals Direct To The Brain, Deadens Pain Impulses
16 Apr 2009
The specialised nerve fibres in the skin are called CT nerves (C-tactile) and they travel directly to the areas in the brain that are important in the emergence of feelings.
'Basically the signals that tell the brain that we are being stroked on the skin have their own direct route to the brain, and are not blocked even if the brain is receiving pain impulses from the same area. In fact it's more the opposite, that the stroking impulses are able to deaden the pain impulses,' says Line Löken, postgraduate student in neurophysiology at the Sahlgrenska Academy.
[....]
Each individual nerve fibre is responsible for touch signals from roughly a square centimetre of skin. The research team used a specially-designed robot, which brushed over the exact area of skin for which a particular nerve fibre is responsible. The subjects were also asked to rate how pleasant or unpleasant they found the brushing.
'As the nerve signals that were sent in the CT nerves became more frequent, the subjects reported the experience as being increasingly pleasant. Of the skin nerves that we studied, it was only the CT nerves that had this strong link between the frequency of the signals and how pleasant it felt,' says researcher Johan Wessberg.
Notes:
Journal: Nature Neuroscience
Title of the article: Coding of pleasant touch by unmyelinated afferents in humans
Authors: Line S. Löken, Johan Wessberg, India Morrisson, Francis McGlone, Håkan Olausson
The full text article is available on Nature Neuroscience's web page: http://www.nature.com/neuro/journal/vaop/ncurrent/abs/nn.2312.html
By: Elin Lindström Claessen
"
A Trance of Pleasure
And now for something completely different:
A 2003 study in Epilepsy and Behavior has some descriptions of the ecstatic seizures experienced by some patients with epilepsy.
They include intense erotic and spiritual experiences, feelings of become close to and blending with other people, and some sensations that couldn't be fully captured in words.
I've put some of the descriptions below because they sound absolutely wonderful:
Patient 1
The first seizure occurred during a concert when he was a teenager. He remembers perceiving short moments of an indefinable feeling. Such episodes recurred and a few months later evolved into a GTC [generalized tonic–clonic seizure]. He characterizes these sensations as ‘a trance of pleasure.’ ‘It is like an emotional wave striking me again and again. I feel compelled to obey a sort of phenomenon. These sensations are outside the spectrum of what I ever have experienced outside a seizure.’ He also describes cold shivering, increased muscle tension, and a delicious taste, and he swallows repeatedly. He enjoys the sensations and is absorbed in them in a way that he can barely hear when spoken to. When in a particular, relaxed mood, he can sometimes induce seizures by ‘opening up mentally’ and contracting muscles. He denies any religious aspects of the symptoms. ‘It’s the phenomenon, the feeling, the fit taking control.’ It lasts a few minutes and afterward he is tired with difficulties expressing himself for about 1 hour.Patient 6
This man has a multifaceted symptomatology and a tendency to interpret bodily sensations as supernatural phenomena. Nevertheless, from the beginning of his forties, he experienced distinct, stereotypical attacks with a ‘change of concept of the surrounding world.’ He reports an ‘oscillating erotic sensation, like twinkling polar light’ in his pelvic region and down the inside of his thighs. This is described as different from sexual excitement, more like ‘an erogenous charge of the skin.’ He may also have a clairvoyant feeling of a ‘telepathic contact with a divine power.’ These sensations are of short duration and may be accompanied by faintness and followed by drowsiness. With carbamazepine treatment, the frequency of these attacks has been considerably reduced.Patient 11
The attacks started in his first school year. The experiences are beyond what can be described in words. ‘I can sense the colours red and orange without seeing them. The feeling has an erotic aspect. It starts in the stomach and spreads upwards. It is pleasant, but not similar to ordinary joy. It is like an explosion.’ In the close presence of another person, he can feel a sort of peculiar unification. An intense déjà vu sensation, a queer taste, and ‘gooseflesh’ are also components of the seizures. As a child he was surprised that his friends denied having similar feelings, and he learned to keep them to himself. Sometimes these attacks evolved into CPSs with reduced consciousness and complex automatisms and afterward he had transient difficulties speaking. Before the diagnosis of epilepsy was made in his late teens, he was referred to a psychiatrist. A right-sided temporal lobe calcification was diagnosed by computed tomography at about 30 years, but he refused surgery. At 42, an expansion in the same region was found by MRI, and he was operated for an anaplastic oligodendroglioma. He was seizure-free for 6 years until recurrence of the tumor.One of the striking things about epilepsy is how different each person's experience of having a seizure can be.
While it is stereotypically assumed to be a negative experience, some aspects can be remarkably beautiful.
The Russian author Dostoyevsky famously said of his epilepsy 'I would experience such joy as would be inconceivable in ordinary life - such joy that no one else could have any notion of. I would feel the most complete harmony in myself and in the whole world and this feeling was so strong and sweet that for a few seconds of such bliss I would give ten or more years of my life, even my whole life perhaps.'
There are several more case descriptions in the article, all of which have some aspect which touch at least the edge of ecstasy, if not the very heart of the experience.
"
Link to article.
Link to PubMed entry for same.
(Via Mind Hacks.)
Another new paper by me: Privation Theories of Pain
Yep. More from me. This time in a philosophy of religion journal --guess I'm branching out.
Privation Theories of Pain
Most modern writers accept that a privation theory of evil should explicitly account for the evil of pain. But pains are quintessentially real. The evil of pain does not seem to lie in an absence of good. Though many directly take on the challenges this raises, the metaphysics and axiology of their answers is often obscure. In this paper I try to straighten things out. By clarifying and categorizing the possible types of privation views, I explore the ways in which privationists about evil are—or should or could be—privationists about pain’s evil.
International Journal for Philosophy of Religion (2009)
DOI: 10.1007/s11153-009-9202-4
http://www.springerlink.com/content/644751l635n21r71/
Super awesome paper: Pain's Evils
Okay. I'm lying. It isn't really super awesome. But it is a new paper by me in the latest issue of the journal Utilitas:
Pain's Evils
The traditional accounts of pain’s intrinsic badness assume a false view of what pains are. Insofar as they are normatively significant, pains are not just painful sensations. A pain is a composite of a painful sensation and a set of beliefs, desires, emotions, and other mental states. A pain’s intrinsic properties can include inter alia depression, anxiety, fear, desires, feelings of helplessness, and the pain’s meaning. This undermines the traditional accounts of pain’s intrinsic badness. Pain is intrinsically bad in two distinct and historically unnoticed ways. First, most writers hold that pain’s intrinsic badness lies either in its unpleasantness or in its being disliked. Given my wider conception of pain, I believe it is both. Pain’s first intrinsic evil lies in a conjunction of all the traditional candidates for its source. Pain’s second intrinsic evil lies in the way it necessarily undermines the self-control necessary for intrinsic goods like autonomy.
Utilitas Vol. 21 No. 2 June 2009
doi:10.1017/S0953820809003550
More drugs, please: Italian edition
May I have your attention please?
Ahem.
STOP DENYING CANCER PATIENTS THE MEDICINE THEY NEED.
Thank you for your attention
Br J Cancer. 2009 Apr 28;
Apolone G, Corli O, Caraceni A, Negri E, Deandrea S, Montanari M, Greco MTMost patients with advanced or metastatic cancer experience pain and despite several guidelines, undertreatment is well documented. A multicenter, open-label, prospective, non-randomised study was launched in Italy in 2006 to evaluate the epidemiology, patterns and quality of pain care of cancer patients. To assess the adequacy of analgesic care, we used a standardised measure, the pain management index (PMI), that compares the most potent analgesic prescribed for a patient with the reported level of the worst pain of that patient together with a selected list of clinical indicators. A total of 110 centres recruited 1801 valid cases. 61% of cases were received a WHO-level III opioid; 25.3% were classified as potentially undertreated, with wide variation (9.8-55.3%) according to the variables describing patients, centres and pattern of care. After adjustment with a multivariable logistic regression model, type of recruiting centre, receiving adjuvant therapy or not and type of patient recruited (new or already on follow-up) had a significant association with undertreatment. Non-compliance with the predefined set of clinical indicators was generally high, ranging from 41 to 76%. Despite intrinsic limitations of the PMI that may be considered as an indicator of the poor quality of cancer pain care, results suggest that the recourse to WHO third-level drugs still seems delayed in a substantial percentage of patients. This delay is probably related to several factors affecting practice in participating centres and suggests that the quality of cancer pain management in Italy deserves specific attention and interventions aimed at improving patients' outcomes.British Journal of Cancer advance online publication, 28 April 2009; doi:10.1038/sj.bjc.6605053 www.bjcancer.com."
(Via HubMed - pain.)
Translating nociceptive processing into human pain models.
Limits on pain models:
Translating nociceptive processing into human pain models.: "
Exp Brain Res. 2009 Apr 29;
Schmelz MAs volunteers can easily communicate quality and intensity of painful stimuli, human pain models appear to be ideally suited to test analgesic compounds, but also to study pain mechanisms. Acute stimulation of nociceptors under physiologic conditions has proven not to be of particular use as an experimental pain model. In contrast, if the experimental models include sensitization of the peripheral or central pain processing they may indeed mimic certain aspects of chronic pain conditions. Peripheral inflammatory conditions can be induced experimentally with sensitization patterns correlating to clinical inflammatory pain. There are also well-characterized models of central sensitization, which mimic aspects of neuropathic pain patients such as touch evoked allodynia and punctate hyperalgesia. The main complaint of chronic pain patients, however, is spontaneous pain, but currently there is no human model available that would mimic chronic inflammatory or neuropathic pain. Thus, although being helpful for proof of concept studies and dose finding, current human pain models cannot replace patient studies for testing efficacy of analgesic compounds."
(Via HubMed - pain.)
01 May 2009
Acupuncture
Proof that acupuncture works – up to a point
By Nic Fleming, Health Correspondent
Last Updated: 12:55am GMT 21/12/2004
Acupuncture significantly reduces pain and improves function in those suffering osteoarthritis of the knee, according to research published yesterday.
Patients who underwent the ancient Chinese needle treatment reported a 44 per cent average reduction in pain and a 40 per cent improvement in mobility.
Acupuncture
‘We have demonstrated that Chinese acupuncture is an effective complement to arthritis treatment’
While acupuncture has been gaining mainstream acceptance, particularly for pain relief, over the last decade the latest study is one of the largest and longest to show such conclusive effects.
Brian Berman, of the University of Maryland School of Medicine, Baltimore, said: "We have demonstrated that traditional Chinese acupuncture is an effective complement to conventional arthritis treatment and can be successfully employed as part of a multi-disciplinary approach to treating the symptoms of osteoarthritis." Acupuncture, which is at least 2,000 years old, is based on the idea that energy flows along channels called meridians in the body.
Practitioners say they block or stimulate these channels by inserting thin needles at precise points. Some have suggested the ancient treatment works by influencing the body's electromagnetic fields.
In Prof Berman's study, a group of 570 patients aged 50 or older suffering from osteoarthritis of the knee was split into 190 who received acupuncture, 191 who received a sham treatment simulating acupuncture and 189 who attended self-help lessons.
advertisement
The volunteers were assessed at four, eight, 14 and 16 weeks. After eight weeks, participants receiving acupuncture were showing an improvement in mobility and by 14 weeks a significant decrease in pain.
They continued to receive standard medical care including non-steroidal anti-inflammatory drugs and pain relievers. By the end of the trials, the reported reduction in pain among those who had acupuncture was 44 per cent, 28 per cent for those who had sham treatment, and around 19 per cent for the self-help group.
The improvements in mobility were 40 per cent for those who had acupuncture, 33 per cent for the control group, and 20 per cent for the self-helpers.
Previous research into the effectiveness of acupuncture has been criticised because of the difficulty of faking needle insertion and therefore providing a general control group.
The research, published in the American journal the Annals of Internal Medicine, was funded by two groups who are part of the National Institutes of Health in the United States.
Dr Stephen Straus, the director of the National Centre for Complementary and Alternative Medicine, said: "For the first time, a clinical trial with sufficient rigour, size and duration has shown that acupuncture reduces the pain and functional impairment of osteoarthritis of the knee."
Dr Stephen Katz, the director of National Institute of Arthritis and Musculoskeletal and Skin Diseases, said: "This disease is one of the most frequent causes of physical disability among adults."
Three in 10 adults in Britain suffer some form of arthritis or joint pain, and two million patients visited their GPs complaining of osteoarthritis this year.
A separate British study, also published in the Annals of Internal Medicine yesterday, indicated that needle treatment appeared to help reduce neck pain.
George Lewith, a senior research fellow at the University of Southampton, found that in a group of 124 patients aged 18 to 80 those given acupuncture over 12 weeks reported a 72 per cent drop in neck pain, while those given sham treatment reported a 60 per cent reduction.
Dr Lewith said: "Our study implies that most of the improvement gained from acupuncture was not due to the needling process itself but due predominantly to the non-specific yet powerful effects which are probably part of the treatment process.
"Acupuncture is safe and effective in reducing pain. It also reduces the intake of pain-killers – important in diminishing unwanted side-effects."
Link
By Nic Fleming, Health Correspondent
Last Updated: 12:55am GMT 21/12/2004
Acupuncture significantly reduces pain and improves function in those suffering osteoarthritis of the knee, according to research published yesterday.
Patients who underwent the ancient Chinese needle treatment reported a 44 per cent average reduction in pain and a 40 per cent improvement in mobility.
Acupuncture
‘We have demonstrated that Chinese acupuncture is an effective complement to arthritis treatment’
While acupuncture has been gaining mainstream acceptance, particularly for pain relief, over the last decade the latest study is one of the largest and longest to show such conclusive effects.
Brian Berman, of the University of Maryland School of Medicine, Baltimore, said: "We have demonstrated that traditional Chinese acupuncture is an effective complement to conventional arthritis treatment and can be successfully employed as part of a multi-disciplinary approach to treating the symptoms of osteoarthritis." Acupuncture, which is at least 2,000 years old, is based on the idea that energy flows along channels called meridians in the body.
Practitioners say they block or stimulate these channels by inserting thin needles at precise points. Some have suggested the ancient treatment works by influencing the body's electromagnetic fields.
In Prof Berman's study, a group of 570 patients aged 50 or older suffering from osteoarthritis of the knee was split into 190 who received acupuncture, 191 who received a sham treatment simulating acupuncture and 189 who attended self-help lessons.
advertisement
The volunteers were assessed at four, eight, 14 and 16 weeks. After eight weeks, participants receiving acupuncture were showing an improvement in mobility and by 14 weeks a significant decrease in pain.
They continued to receive standard medical care including non-steroidal anti-inflammatory drugs and pain relievers. By the end of the trials, the reported reduction in pain among those who had acupuncture was 44 per cent, 28 per cent for those who had sham treatment, and around 19 per cent for the self-help group.
The improvements in mobility were 40 per cent for those who had acupuncture, 33 per cent for the control group, and 20 per cent for the self-helpers.
Previous research into the effectiveness of acupuncture has been criticised because of the difficulty of faking needle insertion and therefore providing a general control group.
The research, published in the American journal the Annals of Internal Medicine, was funded by two groups who are part of the National Institutes of Health in the United States.
Dr Stephen Straus, the director of the National Centre for Complementary and Alternative Medicine, said: "For the first time, a clinical trial with sufficient rigour, size and duration has shown that acupuncture reduces the pain and functional impairment of osteoarthritis of the knee."
Dr Stephen Katz, the director of National Institute of Arthritis and Musculoskeletal and Skin Diseases, said: "This disease is one of the most frequent causes of physical disability among adults."
Three in 10 adults in Britain suffer some form of arthritis or joint pain, and two million patients visited their GPs complaining of osteoarthritis this year.
A separate British study, also published in the Annals of Internal Medicine yesterday, indicated that needle treatment appeared to help reduce neck pain.
George Lewith, a senior research fellow at the University of Southampton, found that in a group of 124 patients aged 18 to 80 those given acupuncture over 12 weeks reported a 72 per cent drop in neck pain, while those given sham treatment reported a 60 per cent reduction.
Dr Lewith said: "Our study implies that most of the improvement gained from acupuncture was not due to the needling process itself but due predominantly to the non-specific yet powerful effects which are probably part of the treatment process.
"Acupuncture is safe and effective in reducing pain. It also reduces the intake of pain-killers – important in diminishing unwanted side-effects."
Link
21 March 2009
Pain in infants and very young children
Interesting. Though, as always, these neurological facts don't by themselves entail any ethical conclusions. Of course, it would be nice to see standard practice err on the side of preventing as much pain as is clinically feasible.
"Pain, Hurt, and Harm: The Ethics of Pain Control in Infants and Children" in The New England Journal of Medicine (Vol. 331.8):
Many myths about pain in children have been discredited. One myth was the belief that very young infants do not have the neurologic capacity to experience pain. Neuroanatomical studies, however, have shown that by 29 weeks of gestation, pain pathways and the cortical and subcortical centers involved in the perception of pain are well developed, as are the neurologic systems for the transmission and modulation of painful sensations 15. Behavioral16,17 and physiologic18 studies have shown that even very young infants respond to painful stimuli. Premature infants undergoing surgery with minimal anesthesia, which was once standard practice, have significantly higher stress responses (by hormonal and metabolic measures) and significantly higher rates of complications and mortality than those given deeper anesthesia.19,20
A related misunderstanding is the belief that even if very young children experience pain, they have no memory of it, and therefore it has no lasting effect. However, recent studies have concluded that pain and distress, such as those associated with circumcision, can endure in memory, resulting, for example, in disturbances of feeding, sleeping, and the stability of the state of arousal.21 Preliminary data even suggest that early experiences of pain may produce permanent structural and functional reorganization of developing nociceptive neural pathways, which in turn may affect future experiences of pain.22
20 January 2009
Tonight's House M.D.
SPOILER ALERT!
----I can't put posts below the fold with blogger so please stop reading if you haven't seen it----
So, I cringed just slightly when I saw that tonight's episode of House M.D. involved a patient with undiagnosable chronic pain. I know it's just a TV show. But my nerdiness won't allow me to avoid comment....
And, as per usual, at least in the way they were described, the partial theories of what his affliction might be were rather dodgy. But whatever. Here's my nerdy question: wouldn't the symptoms have been alleviated earlier in treatment?
The final diagnosis was some weird form of epilepsy that 'rewired the pain neurons of certain areas of the brain'. But nowadays several anticonvulsants (at least atypical anticonvulsants) like Neurotin, Lamictal, and friends,are commonly used relatively early in treating all sorts of chronic pain.
And, in many cases, treatment for chronic (or severe acute) pain includes benzodiazapenes like Lorazepam, which also have anticonvulsant properties.
Finally, if they had really suspected that the problem was opiate-blowback, wouldn't House's team have used at least some of the above in tandem with the Naloxone to alleviate the suckiness of flushing the opiates from the patient's system?
Okay. I know. Just a TV show. Back to regularly scheduled programming...
----I can't put posts below the fold with blogger so please stop reading if you haven't seen it----
So, I cringed just slightly when I saw that tonight's episode of House M.D. involved a patient with undiagnosable chronic pain. I know it's just a TV show. But my nerdiness won't allow me to avoid comment....
And, as per usual, at least in the way they were described, the partial theories of what his affliction might be were rather dodgy. But whatever. Here's my nerdy question: wouldn't the symptoms have been alleviated earlier in treatment?
The final diagnosis was some weird form of epilepsy that 'rewired the pain neurons of certain areas of the brain'. But nowadays several anticonvulsants (at least atypical anticonvulsants) like Neurotin, Lamictal, and friends,are commonly used relatively early in treating all sorts of chronic pain.
And, in many cases, treatment for chronic (or severe acute) pain includes benzodiazapenes like Lorazepam, which also have anticonvulsant properties.
Finally, if they had really suspected that the problem was opiate-blowback, wouldn't House's team have used at least some of the above in tandem with the Naloxone to alleviate the suckiness of flushing the opiates from the patient's system?
Okay. I know. Just a TV show. Back to regularly scheduled programming...
10 November 2008
Expectation and uncertainty on pain ratings
Modulation of pain ratings by expectation and uncertainty: Behavioral characteristics and anticipatory neural correlates
Christopher A. Browna, Ben Seymourb, Yvonne Boylea, Wael El-Deredyc and Anthony K.P. Jonesa
ScienceDirect - Pain : Modulation of pain ratings by expectation and uncertainty: Behavioral characteristics and anticipatory neural correlates
Christopher A. Browna, Ben Seymourb, Yvonne Boylea, Wael El-Deredyc and Anthony K.P. Jonesa
Expectations about the magnitude of impending pain exert a substantial effect on subsequent perception. However, the neural mechanisms that underlie the predictive processes that modulate pain are poorly understood. In a combined behavioral and high-density electrophysiological study we measured anticipatory neural responses to heat stimuli to determine how predictions of pain intensity, and certainty about those predictions, modulate brain activity and subjective pain ratings. Prior to receiving randomized laser heat stimuli at different intensities (low, medium or high) subjects (n = 15) viewed cues that either accurately informed them of forthcoming intensity (certain expectation) or not (uncertain expectation). Pain ratings were biased towards prior expectations of either high or low intensity. Anticipatory neural responses increased with expectations of painful vs. non-painful heat intensity, suggesting the presence of neural responses that represent predicted heat stimulus intensity. These anticipatory responses also correlated with the amplitude of the Laser-Evoked Potential (LEP) response to painful stimuli when the intensity was predictable. Source analysis (LORETA) revealed that uncertainty about expected heat intensity involves an anticipatory cortical network commonly associated with attention (left dorsolateral prefrontal, posterior cingulate and bilateral inferior parietal cortices). Relative certainty, however, involves cortical areas previously associated with semantic and prospective memory (left inferior frontal and inferior temporal cortex, and right anterior prefrontal cortex). This suggests that biasing of pain reports and LEPs by expectation involves temporally precise activity in specific cortical networks.
ScienceDirect - Pain : Modulation of pain ratings by expectation and uncertainty: Behavioral characteristics and anticipatory neural correlates
25 October 2008
Heat and pain
Hot.
ScienceDaily (Jul. 5, 2006)
The old wives’ tale that heat relieves abdominal pain, such as colic or menstrual pain, has been scientifically proven by a UCL (University College London) scientist, who will present the findings today at the Physiological Society’s annual conference hosted by UCL.
Dr Brian King, of the UCL Department of Physiology, led the research that found the molecular basis for the long-standing theory that heat,such as that from a hot-water bottle applied to the skin, provides relief from internal pains, such as stomach aches, for up to an hour.
Dr King said: “The pain of colic, cystitis and period pain is caused by a temporary reduction in blood flow to or over-distension of hollow organs such as the bowel or uterus, causing local tissue damage and activating pain receptors.
“The heat doesn’t just provide comfort and have a placebo effect – it actually deactivates the pain at a molecular level in much the same way as pharmaceutical painkillers work. We have discovered how this molecular process works.”
If heat over 40 degrees Celsius is applied to the skin near to where internal pain is felt, it switches on heat receptors located at the site of injury. These heat receptors in turn block the effect of chemical messengers that cause pain to be detected by the body.
The team found that the heat receptor, known as TRPV1, can block P2X3 pain receptors. These pain receptors are activated by ATP, the body’s source of energy, when it is released from damaged and dying cells. By blocking the pain receptors, TRPV1 is able to stop the pain being sensed by the body.
(2006, July 5). Heat Halts Pain Inside The Body. ScienceDaily. Retrieved March 19, 2008, from http://www.sciencedaily.com /releases/2006/07/060705090603.htm
28 September 2008
Trying to control pain
Interesting.
Wellcome Trust (2006, November 2). Trying To Control Pain Can Be A Double-edged Sword, Say Scientists. ScienceDaily. Retrieved March 19, 2008, from http://www.sciencedaily.com /releases/2006/10/061031191327.htm
Trying To Control Pain Can Be A Double-edged Sword, Say Scientists
ScienceDaily (Nov. 2, 2006) — Scientists have shown for the first time why a feeling of control helps us reduce pain.....Using fMRI scanners, which allow scientists to examine how the brain operates, the research, led by Dr Katja Wiech and Dr Raffael Kalisch, showed that when people feel that they can control their pain, an area of their prefrontal cortex associated with a feeling of security is activated. The findings are published in the Journal of Neuroscience today and have been welcomed by the Expert Patients Programme.
More significantly, the team went on to show that when faced with pain beyond their control, people who tend to feel more in control of their own lives show a lower response in the prefrontal cortex, indicating that they are less effective in coping with pain than those who don't expect to have control.
"Patients with persistent pain report that often it is not the pain itself that makes their situation unbearable, but the fact that there is nothing they can do against it which makes them feel helpless," explains Dr Wiech. "Unfortunately, this feeling of uncontrollability in turn tends to worsen the pain. On the other hand, teaching persistent pain patients psychological coping strategies to handle their pain usually does help reduce its effects."
Dr Wiech and her team set up an experiment to investigate how people cope with pain. In the first stage, volunteers were given an electric stimulus to the backs of their hands and told that they could stop the pain at any point. In the second stage, they were told that the decision to stop the pain was out of their control and could only be stopped by a person or computer outside the room.
Using one of the centre's fMRI scanners, the researchers were able to show that a number of areas of the brain were activated according to whether the volunteer felt in control of the pain. Most important was the anterolateral prefrontal cortex, which is associated with successful coping with feelings of anxiety.
The findings may have implications for future therapeutics, believes Dr Wiech.
"If we were able to stimulate the prefrontal cortex through psychological intervention, medication or some other stimulus, we could help reduce the pain felt by a patient," she says. "However, we are still some way of this."
The team also analysed the subjects' outlook on life, examining whether they felt in control of their own lives. They found that whilst the subjects' outlook did not affect the anterolateral prefrontal cortex when they controlled the stimulus, when they were not able to stop the painful stimulation subjects with no control expectations were better at activating this brain region than those with a strong control belief.
The findings support the practice of "acceptance-based therapy" whereby doctors focus on training patients to cope with the pain rather than attempting to make the pain go away.
"Throughout our lives, we are taught that we should aim to take control of our lives, to get the best job, find the best partner," says Dr Wiech. "But sometimes we should accept what we have and make the most of it. Rather than constantly battling pain, our research supports the view that it is better to provide a patient with the tools to cope with his or her persistent pain."
The findings are welcomed by Pete Moore, lead trainer in pain management for the Expert Patients Programme Community Interest Company.
"This is interesting work by UCL. We have found that many people with pain are over achievers and tend to do more than they have to. This is why when people with persistent pain attend an Expert Patients Programme they are provided with a toolbox of self-management skills to support them to manage their day-to-day pain."
Wellcome Trust (2006, November 2). Trying To Control Pain Can Be A Double-edged Sword, Say Scientists. ScienceDaily. Retrieved March 19, 2008, from http://www.sciencedaily.com /releases/2006/10/061031191327.htm
09 September 2008
27 August 2008
Suit of Armour
Skevington notes:
By supplying lists of pain adjectives, practitioners and researchers are effectively teaching their patients a pain language that...provides a legitimate lexicon that may be recycled in later consultations as the 'correct' descriptor to use. By supplying the words and following the prescribed instructions, we blinker ourselves to our patients' ability to describe pain in their own varied language, which in many cases is not reducible to a single word in the English language. For example, a patient with early synovitis who was asked to describe her pain said, 'it is like a suit of armour which is too tight'. The author is still struggling to translate this into a single descriptor from the McGill Pain Questionnaire. [p.52]
18 August 2008
Pain and self control
As some of you know, one of my abiding research interests is the relationship between pain and self-control. Thus I bring you this:
A scientist developing a prosthetic pain detection system to help lepers who had lost sensation in their limbs avoid damage describes its failure:
In the end we had to abandon the entire scheme. Most important, we found no way around the fundamental weakness in our system: it remained under the patient's control. If the patient did not want to heed the warnings from our sensors, he could always find a way to bypass the whole system. Why must pain be unpleasant? Why must pain persist? Our system failed for the precise reason that we could not effective duplicate those two qualities of pain. They mysterious power of the human brain can force a person to STOP! --something I could never accomplish with my substitute system. And 'natural' pain will persist as long as danger threatens, whether we want it to or not, unlike my substitute system, it cannot be switched off."
Brand, P. and P. Yancey. 1993. Pain: The Gift Nobody Wants. New York: Harper Collins. Pp.195-186
08 August 2008
Marijuana and HIV Neuropathic Pain
From the always informative Science Daily:
ScienceDaily (Aug. 7, 2008) — In a double-blind, placebo-controlled clinical trial to assess the impact of smoked medical cannabis, or marijuana, on the neuropathic pain associated with HIV, researchers at the University of California, San Diego School of Medicine found that reported pain relief was greater with cannabis than with a placebo.
[....]
The proportion of subjects achieving pain reduction of 30 percent or more was greater for those smoking cannabis than those smoking the placebo.
"Neuropathy is a chronic and significant problem in HIV patients as there are few existing treatments that offer adequate pain management to sufferers," Ellis said. "We found that smoked cannabis was generally well-tolerated and effective when added to the patient's existing pain medication, resulting in increased pain relief."
[....]Using verbal descriptors of pain magnitude, cannabis was associated with an average reduction of pain intensity from 'strong' 'to mild-to-moderate' in cannabis smokers, according to Ellis. Also, cannabis was associated with a sizeable (46% versus 18% for placebo) proportion of patients reporting clinically meaningful pain relief.
The study's findings are consistent with and extend other recent research supporting the short-term efficacy of cannabis for neuropathic pain, also sponsored by the CMCR.
"This study adds to a growing body of evidence that indicates that cannabis is effective, in the short-term at least, in the management of neuropathic pain," commented Igor Grant, M.D., professor of psychiatry and director of the CMCR.
Grant noted that this is the fourth CMCR sponsored study to provide convergent evidence that cannabis can help in relieving these types of pain.
Link
30 July 2008
July Pain Carnival
July's Pain-Blog Carnival is up:
http://www.howtocopewithpain.org/blog/261/july-pain-blog-carnival/
Lots of good stuff as usual.
http://www.howtocopewithpain.org/blog/261/july-pain-blog-carnival/
Lots of good stuff as usual.
19 May 2008
Acupuncture
http://www.telegraph.co.uk/news/main.jhtml;jsessionid=G4FNO0Z2UCNWVQFIQMGSFF4AVCBQWIV0?xml=/news/2005/05/02/nacup02.xml
Needle cure effect 'is not all in the mind'
By Catriona Davies
Last Updated: 12:30am BST 02/05/2005
Acupuncture has a genuine ability to relieve pain, scientists have found.
Many scientists and doctors had believed that any benefit from acupuncture was purely psychological because patients expected an improvement in their health.
Undergoing acupuncture
Acupuncture has been gaining popularity in Britain but still divides medical opinion
Now a study has found that the brain responses to real acupuncture are different from those from a placebo.
Acupuncture, an ancient Chinese treatment which involves sticking needles in the skin, has been gaining popularity in Britain but still divides medical opinion.
Dr George Lewith, who led a team of researchers at Southampton University and University College London, said acupuncture showed similar results to drug treatments for other chronic benign conditions.
Using prozac to treat depression, for example, was successful in 80 per cent of patients prescribed the drug. Dr Lewith said in most cases, the improvement was purely that the patient expected improvement. But in 10 per cent, the improvement came from real treatment beyond that of a placebo.
Clinical trials of acupuncture showed similar results.
In a study published today in the journal Nature, Dr Lewith's team gave each of 14 patients with arthritis in their thumbs three different treatments in a random order.
Patients received real acupuncture, treatment with "stage dagger" needles which retracted into their handle rather than penetrating skin, or treatment with blunt needles which did not penetrate patients' skin.
Scientists found activity in different brain areas for each treatments. Both the real and placebo treatments triggered activity in the brain known to produce natural opiates, substances that relieve pain.
However, the real treatment also triggered activity in an area of the brain which the placebo did not.
Needle cure effect 'is not all in the mind'
By Catriona Davies
Last Updated: 12:30am BST 02/05/2005
Acupuncture has a genuine ability to relieve pain, scientists have found.
Many scientists and doctors had believed that any benefit from acupuncture was purely psychological because patients expected an improvement in their health.
Undergoing acupuncture
Acupuncture has been gaining popularity in Britain but still divides medical opinion
Now a study has found that the brain responses to real acupuncture are different from those from a placebo.
Acupuncture, an ancient Chinese treatment which involves sticking needles in the skin, has been gaining popularity in Britain but still divides medical opinion.
Dr George Lewith, who led a team of researchers at Southampton University and University College London, said acupuncture showed similar results to drug treatments for other chronic benign conditions.
Using prozac to treat depression, for example, was successful in 80 per cent of patients prescribed the drug. Dr Lewith said in most cases, the improvement was purely that the patient expected improvement. But in 10 per cent, the improvement came from real treatment beyond that of a placebo.
Clinical trials of acupuncture showed similar results.
In a study published today in the journal Nature, Dr Lewith's team gave each of 14 patients with arthritis in their thumbs three different treatments in a random order.
Patients received real acupuncture, treatment with "stage dagger" needles which retracted into their handle rather than penetrating skin, or treatment with blunt needles which did not penetrate patients' skin.
Scientists found activity in different brain areas for each treatments. Both the real and placebo treatments triggered activity in the brain known to produce natural opiates, substances that relieve pain.
However, the real treatment also triggered activity in an area of the brain which the placebo did not.
19 March 2008
Fibromyalgia and pain memory
This is old, but useful.
ScienceDaily (2000-11-01) -- The symptoms of fibromyalgia may be the result of a central nervous system that "remembers" pain sensations for an abnormally long time, according to research presented at the American College of Rheumatology Annual Scientific Meeting Oct. 29 -- Nov. 2 in Philadelphia, Pennsylvania.
Link
18 March 2008
Being realistic about labor pain
Interesting.
ScienceDaily (Mar. 17, 2008) — A pain-free and drug-free labour may be many expectant mothers' dream but a review in the open access journal BMC Medicine reveals that reality hits hard. Most women's labour experiences differ markedly from their expectations. They are often ill-prepared for what might happen and consequently may be disappointed when the birth does not "go to plan".LinkThe study's authors conclude that antenatal programmes should "get real". "People involved in antenatal care should listen to women's hopes for labour whilst also preparing them for what might actually happen during labour," said Joanne Lally of Newcastle University, who led the investigation. "Plans for a labour free of pain relief need to be complemented by preparing women for the possibility that they might need pain relief. Education can help to fill the gap between expectation and experience and thus ensure women are realistically prepared for their birthing experience."
The research team from Newcastle University studied published literature on women's expectations and experience of pain and pain relief in labour. They found that a gap exists between expectations and experience in four key areas: the level and type of pain, access to pain relief, the level of participation in and control over decision--making, and the level of control during labour.
Most of the literature reviewed showed that women underestimate the intensity of the pain they will experience and sometimes hold an unrealistic ideal for a drug-free labour. Indeed, in one study, more than half of the women interviewed who said they would not use pain relief actually did use it.
"Our analysis highlights the importance of antenatal education. It can empower women to have realistic expectations and make informed decisions," notes the author.
"If women can be better educated they can express their preferences but also be aware that things may not always go to plan. They can then be prepared for different eventualities and so make more realistic decisions and have a better experience."
Birth plans or other decision aids can assist women when making decisions about pain relief in labour, but evidence suggests these are not widely used. Recent guidelines published by the National Institute for Clinical Excellence (NICE) call for more research into how health professionals can effectively support pregnant women in making informed decisions about labour.
Journal reference: More in hope than expectation: Women's experience and expectations of pain relief in labour: A review. Joanne E Lally, Madeleine J Murtagh, Sheila Macphail and Richard G Thomson. BMC Medicine (in press)
Adapted from materials provided by BioMed Central, via EurekAlert!, a service of AAAS.
05 March 2008
BLEG: Opiates and renal failure
Hi all,
As I mentioned, I'm suddenly in the position of helping coordinate my grandpa's palliative care. Since I'm not a clinician, I need to get up to speed on some of the pharmacology so that I can have meaningful discussions with the real doctors.
Thus I'd really appreciate it if you could point me in the right direction toward any resources on treating acute pain in patients with severe renal impairment/failure.
Here's an example of the sort of information I'm looking for:
After reading through a bunch of journals early this morning, it seems like there's pretty good reason to not give people with severe renal impairment/failure morphine or hydromorphone. Two of the metabolites don't clear very well and can build up to cause coma or respiratory failure (in fact, at least one of the dangerous metabolites --6MG I think-- doesn't really affect pain, so the danger well outlasts the analgesic effect of the dose).
Codeine is probably even worse. The evidence with oxycodone isn't entirely clear; fentanyl is probably okay. But methadone seems to be all around pretty safe.
These are just my impressions from a bunch of journal articles. But I feel like I can now intelligibly ask his doctors whether they might consider trying methadone instead of giving him morphine for breakthrough pains and then giving him nothing (occasionally APAP) for very long periods. I don't want to second-guess their judgment, but I do want to be able to understand the treatment options....
I'll appreciate anything you can recommend.
Thanks again.
[also, sorry that these posts are pretty sloppy. I'm posting from my phone outside the hospital.]
As I mentioned, I'm suddenly in the position of helping coordinate my grandpa's palliative care. Since I'm not a clinician, I need to get up to speed on some of the pharmacology so that I can have meaningful discussions with the real doctors.
Thus I'd really appreciate it if you could point me in the right direction toward any resources on treating acute pain in patients with severe renal impairment/failure.
Here's an example of the sort of information I'm looking for:
After reading through a bunch of journals early this morning, it seems like there's pretty good reason to not give people with severe renal impairment/failure morphine or hydromorphone. Two of the metabolites don't clear very well and can build up to cause coma or respiratory failure (in fact, at least one of the dangerous metabolites --6MG I think-- doesn't really affect pain, so the danger well outlasts the analgesic effect of the dose).
Codeine is probably even worse. The evidence with oxycodone isn't entirely clear; fentanyl is probably okay. But methadone seems to be all around pretty safe.
These are just my impressions from a bunch of journal articles. But I feel like I can now intelligibly ask his doctors whether they might consider trying methadone instead of giving him morphine for breakthrough pains and then giving him nothing (occasionally APAP) for very long periods. I don't want to second-guess their judgment, but I do want to be able to understand the treatment options....
I'll appreciate anything you can recommend.
Thanks again.
[also, sorry that these posts are pretty sloppy. I'm posting from my phone outside the hospital.]
Well, this sucks....
My 89 year old grandpa has graciously decided to allow me to put my several years of dilettantism with the pain sciences into practice. He's entered the hospital in pretty dire straights. I'm trying to help my parents be involved with decisions about his palliative care (without getting in the real clinicians way).
So, I'll be posting some reflections about his/my experiences with pain care, ethical issues, and other topics, as we go. I'm sure much of this will be naive; especially compared with many of your experiences and backgrounds. But perhaps I'll stumble across something interesting or useful to you.
Also, from time to time I'll probably be soliciting advice on where to find information on certain specialized topics. I'll really appreciate any help I can get.
So, I'll be posting some reflections about his/my experiences with pain care, ethical issues, and other topics, as we go. I'm sure much of this will be naive; especially compared with many of your experiences and backgrounds. But perhaps I'll stumble across something interesting or useful to you.
Also, from time to time I'll probably be soliciting advice on where to find information on certain specialized topics. I'll really appreciate any help I can get.
02 March 2008
Awesome.
Might it be that the normalization of torture in our culture has not really been a good thing?
Was torture part of the pep talk?
Suit alleges waterboarding used as motivational technique
By Erin Alberty
The Salt Lake Tribune
Salt Lake Tribune
A supervisor at a motivational coaching business in Provo is accused of waterboarding an employee in front of his sales team to demonstrate that they should work as hard on sales as the employee had worked to breathe.
In a lawsuit filed last month, former Prosper Inc. salesman Chad Hudgens alleges his managers also allowed the supervisor to draw mustaches on employees' faces, take away their chairs and beat on their desks with a wooden paddle "because it resulted in increased revenues for the company."
Prosper President Dave Ellis responded that the allegations amount to "sensationalized" versions of events that have gone uncorroborated by Hudgens' former coworkers.
"They just roll their eyes and say, 'This is ridiculous . . .. That's not how it went down,' '' Ellis said.
The suit claims that Hudgens' team leader, Joshua Christopherson, asked for volunteers in May for "a new motivational exercise," which he did not describe. Hudgens, who was 26 at the time, volunteered in order to "prove his loyalty and determination," the suit claims.
Christopherson led the sales team to the top of a hill near the office and told Hudgens to lie down with his head downhill, the suit claims. Christopherson then told the rest of the team to hold Hudgens by the arms and legs.
Christopherson poured water from a gallon jug over Hudgens' mouth and nostrils - like the interrogation strategy known as waterboarding - and told the team members to hold Hudgens down as he struggled, the suit alleges.
"At the conclusion of his abusive demonstration, Christopherson told the team that he wanted them to work as hard on making sales as Chad had worked to breathe while he was being waterboarded," the suit alleges.
Ellis said the exercise was a dramatization of a story in which a young man asks Socrates to become his teacher. Socrates responds by plunging the student's head underwater and telling him he will learn once his desire for knowledge is as great as his desire to breathe.
However, Ellis said Christopherson explained the exercise before Hudgens volunteered, no one held Hudgens down and Hudgens was free to get up if he was uncomfortable.
"It was meant to be a team-building exercise," Ellis said. "Everybody was . . . involved and enthusiastic."
Hudgens claims he complained to Prosper managers about the exercise, but no action was taken against Christopherson until Hudgens left Prosper.
Prosper attorney George Brunt said Hudgens lodged the complaint six weeks after the exercise; in the meantime, Hudgens joined his team on a water skiing retreat and drove the boat, Brunt said. Ellis said Christopherson was suspended for two weeks while managers investigated Hudgens' complaint. Christopherson returned to work and remains the sales team leader, Ellis said.
"It's incredible to even suggest that he would put anyone under a level of discomfort," Ellis said. "He's a really nice, pleasant, polite young man. He's very dedicated and takes his job very seriously."
However, the suit claims Christopherson "intentionally engaged in physically and emotionally abusive conduct" to punish workers who did not meet company performance goals.
"Prosper's management passed by and through Christopherson's team area and was able to see mustaches on its employees, missing chairs and Christopherson's paddle," the suit alleges. Ellis said no managers have said they saw the activities described in Hudgens' suit, and the employees reported they are "more along the lines of fun."
"It's voluntary, it's humorous, it's team and camaraderie-building," Ellis said.
Hudgens left Prosper because of sleeplessness, anxiety and depression he experienced after the waterboarding, the suit claims. He required psychological counseling for emotional trauma, the suit claims.
The suit accuses Christopherson and Prosper of assault and battery, intentional infliction of emotional distress and wrongful termination. It accuses Christopherson of interfering with Hudgens' employment relationship with Prosper.
Prosper "provides executive-level coaching for individuals," according to its Web site. Personal coaches offer mentoring that focuses on business and finance.
"Our mission is to provide our students with the education and hands-on experiences they need to achieve their personal and professional goals," the Web site claims. "We strive to make the road to personal achievement meaningful, rewarding, and enjoyable."
Link
H/T TPM
Might it be that the normalization of torture in our culture has not really been a good thing?
The Catholic Church on torture
Also from the same Harpers article, the official Catholic Church position on torture:
Respect for bodily integrity.
[2297.] Kidnapping and hostage taking bring on a reign of terror; by means of threats they subject their victims to intolerable pressures. They are morally wrong. Terrorism threatens, wounds, and kills indiscriminately; it is gravely against justice and charity. Torture which uses physical or moral violence to extract confessions, punish the guilty, frighten opponents, or satisfy hatred is contrary to respect for the person and for human dignity. Except when performed for strictly therapeutic medical reasons, directly intended amputations, mutilations, and sterilizations performed on innocent persons are against the moral law.
[2298.] In times past, cruel practices were commonly used by legitimate governments to maintain law and order, often without protest from the Pastors of the Church, who themselves adopted in their own tribunals the prescriptions of Roman law concerning torture. Regrettable as these facts are, the Church always taught the duty of clemency and mercy. She forbade clerics to shed blood. In recent times it has become evident that these cruel practices were neither necessary for public order, nor in conformity with the legitimate rights of the human person. On the contrary, these practices led to ones even more degrading. It is necessary to work for their abolition. We must pray for the victims and their tormentors.
Subscribe to:
Posts (Atom)

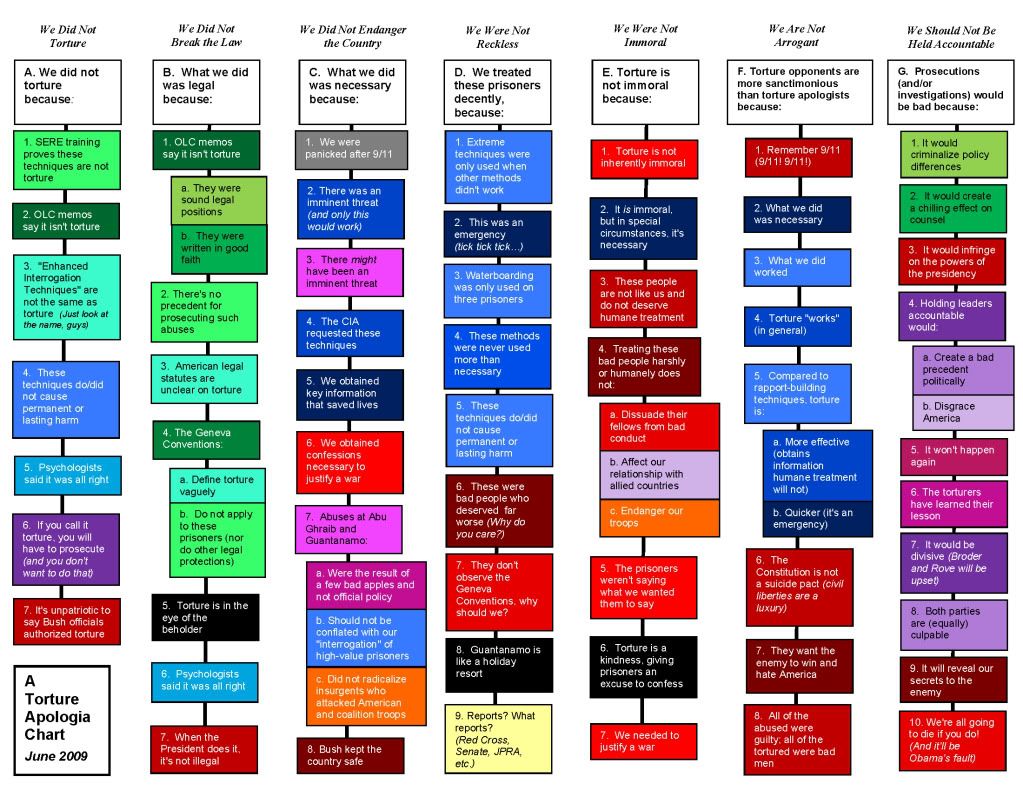{kind=link}